
Advice after your nerve block for surgery
On this page…
You or your relative has been admitted with a periprosthetic fracture
This page has been designed for you by health professionals to provide you and your relatives with information that may help guide you through your hospital stay.
Our aim is for you to regain an appropriate level of function and return to your home environment with a suitable level of assistance.
If your periprosthetic fracture requires surgery then we anticipate a hospital stay of around 2 weeks. However, some patients may recover quicker and others may require a bit more time.
Surgery can improve the pain and allow you to get up and walk. The type of surgery a patient has depends on the type of periprosthetic fracture that has occurred.
What is a periprosthetic fracture?
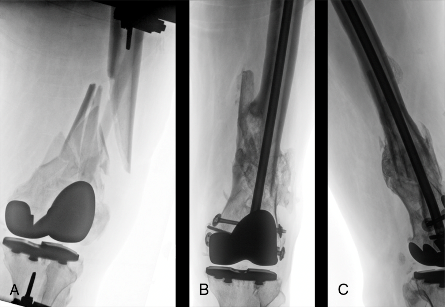
A periprosthetic fracture is a broken bone that happens around or very close to the implants of a hip or knee replacement. This can happen in the top of the femur near where there is a hip implant, (Proximal – Image A). Or near the bottom of the femur where there is a knee implant (Distal – Image B). The location of your fracture can determine the management that the orthopaedic surgeon suggests. It may be deemed that an operation is not needed to manage your fracture - this is referred to as conservative management.


What causes a peri-prosthetic fracture?
Trauma is the main cause of peri-prosthetic fractures. This ranges from car accidents to falling.
Falls are common in older people, and one in three people over 65 will fall each year. As we get older our bones become weaker, making them more prone to breaking. Osteoporosis and other bone diseases can increase the effect of age and further weaken bone.
Due to the increasing number of joint replacements performed in the last 30 years, the number of revision surgeries is growing constantly, particularly in elderly patients. Peri-prosthetic fractures are significantly more common after revision surgery.
Operative management
|
Intramedullary (IM) Nail After periprosthetic fractures around total knee replacements |
|
|
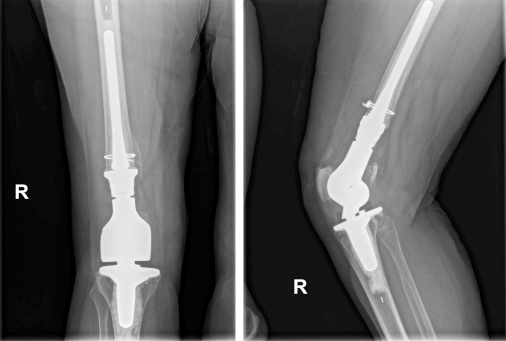
Distal femoral reconstruction (DFR) After periprosthetic fractures around total knee replacements |
|
|
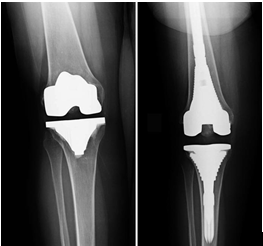
Revision Total Knee Replacement (TKR) After periprosthetic fractures around total knee replacements |
|
|
Open Reduction and Internal Fixation (ORIF) With plates, screw, and cables to hold the bone in place, can be used with hip and knee periprosthetic fractures |
|
|
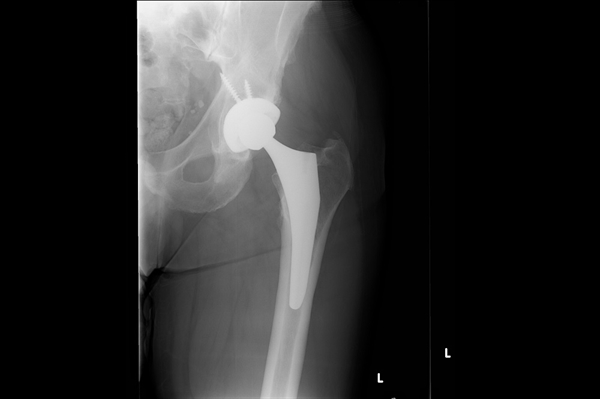
Revision Total hip replacement (THR) After periprosthetic fractures around hip prosthesis |
|
Conservative Management
The doctors looking after you may decide after reviewing your x-rays that they want to treat your injury conservatively (without surgery).
They may decide not to do an operation if your fracture has remained well aligned, or if you have lots of other medical conditions which may put you at high risk of becoming unwell during a operation.
Weight bearing status
The consultant looking after you will make a decision around how much weight you can put through your injured leg. Your Physiotherapist will assist in teaching you how to maintain these weight-bearing statuses.
Below are all the weight-bearing statuses.
- Non weight bearing (NWB) – This means that you can not put any weight through your injured leg. You should keep the foot of your injured leg off the floor
- Limited weight bearing – This means that you have functional restrictions (e.g. no stairs, no sports) or distance restrictions (e.g. indoors only, bed to chair)
- Unrestricted weight bearing – This means there is no restriction in how much weight you can put onto your injured leg. This term can be interchangeable with the term ‘weight bear as tolerated’ (WBAT)
The Anaesthetic
A spinal anaesthetic or general anaesthetic is used during an operation for a peri-prosthetic fracture.
A spinal anaesthetic is when a local anaesthetic drug is injected through a needle into a small space in the back to numb the nerves from the waist downwards. This may be combined with sedation to help relax during the procedure and the operation.
Alternatively, a general anaesthetic may be used. This is when medicines are used to give a state of controlled unconsciousness during the operation. Pain relief may be given by a nerve block or numbing solution around the joint itself prior to the op.
The aim is to reduce the pain and the amount of strong pain killers such as morphine, which can have common side effects of nausea and vomiting, confusion, bladder irritation and constipation.
The Operation
The operation on average takes 60-90 minutes, you will then be taken into recovery to be monitored before being transferred back to the ward. If you would like any further information regarding your operation, please do not hesitate to ask one of the doctors on the ward who will be happy to discuss this with you.
Resuscitation
Many patients who fracture their hip are frail and have many significant underlying health issues. It is not unusual for patients to become more unwell in the recovery period after an operation. We encourage patients and their relatives to discuss with the doctors what their wishes would be, should they become more unwell whilst in hospital.
The doctors routinely discuss resuscitation during the admission process. Resuscitation is where we perform CPR (chest compressions and electric shocks) to re-start the heart after it has stopped (cardiac arrest).
The rate of survival of frail elderly patients who experience a cardiac arrest in hospital is very low, the resuscitation process is very invasive and the risk of brain damage, rib fractures and pneumonia very high. The decision to perform or not perform CPR is a medical decision.
For those who have a ‘Do not attempt CPR’ decision (DNACPR) this does not prevent you from receiving other treatment on the ward such as antibiotics, IV fluids, oxygen therapy or rehab.
Your ward team
You will be looked after on the ward by a variety of health professionals. All members should be wearing an identification badge to help you recognise them.
Here is a brief reference guide of their roles:
Doctors:
- Doctors either wear their own clothes or scrubs.
- You will be admitted under the care of an Orthopaedic Consultant and their team. You will be seen by them following your operation
- If you’re 60 and over, you will be seen by our Consultant Orthogeratrician and their team who specialise in the management of fragility fractures and medical issues in the older person alongside the orthopaedic team.
Nursing Staff:
- The role of a nurse is to administrate medication, assist with personal care and monitor your well-being.
- Nursing staff wear blue trousers and tops in various shades of blue. Ward sister (navy blue), senior sister (navy blue) and junior nurse (pale blue). Health Care Assistants support the nurses (purple).
Physiotherapists:
- The physiotherapist on your ward will get you out of bed the day after your surgery and work with you regularly with the aim to get you on your feet as soon as possible. They will provide you with any mobility aids you may require
- They wear navy blue trousers/shorts and a white polo top or tunic with a navy trim
Occupational Therapists (OT):
- The OT will see you after your surgery and assess your needs to go home
- If they feel you require support at home, they will provide you with or recommend any equipment and help you may need to assist you with this.
- They wear green trousers and a white polo top or tunic with a green trim
Other Ward Staff:
- Pharmacy (green tunics) ensure you have been prescribed appropriate medication and prepare any medication for home.
- Porters (navy blue top and trousers) ensure you get to any areas of the hospital outside of the ward for medical reasons.
- Dieticians (burgundy tunics with light blue trim) will assess your nutritional needs if needed. They are able to advise you on what food and drink you should be consuming, and can provide additional nutritional support if required.
Day 1 post operation
- Your wound will be checked by nurse and/or consultant.
- You will be reviewed by orthopaedic team and by the orthogeriatric team (less than 72 hours from your admission, if over 60).
- You will have a routine blood test and in some cases a X-Ray of your femur.
- You are encouraged to eat and drink normally. It’s important that you keep hydrated to help with recovery.
- You will receive regular pain relief, but you may be written up for additonal pain relief if your pain is severe or to allow you to mobilise more easily. You will need to request this extra pain relief.
- Your bladder and bowel function will be monitored, and your catheter should be removed the day after the operation.
- You will be assessed by a physiotherapist, taught exercises and mobilised out of bed. Once you have been taught the exercises, it is your responsibility to carry these out indepedently if able.
- We encourage patients to be in their own clothes so ask your visitors to bring items such as supportive footwear and comfortable clothing to help promote your recovery.
Day 2 Onwards
- You should be sitting out of bed daily, ready for physiotherapy sessions.
- You will be reviewed by the physiotherapist regularly with the aim to walk further every day.
- If you need to climb stairs at home you will practise this in hospital.
- You should be carrying out your exercises 3 times per day independently if able to.
- You should be getting dressed daily, please ask for help from health care asisstants or nursing staff if needed.
- The OT will assess how you will manage day to day tasks and whether you may need any aids at home should you require assessment.
- Your memory will be assessed and you will be monitored for acute confusion, about half of people with a femur fracture already have memory problems or become temporarily confused (delirium).
- Your risk of further falls will be assessed and acted upon (medication review, strength and balance exercises, occupational therapist assessment)
- Your risk of osteoporosis will also be assessed and you may be started on bone protection (vitamin D, calcium, bisphosphonates), sent for a special scan of your bones or referred to the outpatient rheumathology clinic for follow up.
Leaving the hospital
- Following your operation we aim to discharge you home from hospital as soon as you are medically stable and safe to continue your recovery at home.
- The doctors will need to declare you as medically stable for discharge prior to going home and provide you with discharge letters. This may happen at a different time to when the physiotherapy and occupational therapy team deem you safe to return home.
- Depending on your mobility, you will need to discuss transport to get home, if you need assistance the nurses can help arrange this
- Pharmacy will arrange your medication for going home.
- Any follow up referrals will be made upon your discharge.
- If help is required at home for personal and domestic care, this will be put in place prior to your discharge from hospital. However, some patients may need a period of time in a step-down hospital in their local area prior to going home to progress with their independence.
- Your discharge plans may change as you improve whilst you are on the ward. These plans are made by the professionals that work alongside you and have assessed your needs, however this will be discussed with you and your family at the time.
Contact us
If you have any queries relating to this information, please contact the Orthopaedics service.
About this information
Service:
Orthopaedics
Reference:
BB/112
Approval date:
1 April 2026
Review date:
1 April 2029
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.