Advice after your nerve block for surgery
On this page…
Introduction
You are having, or may have had, fenestrated endovascular (FEVAR) surgery to repair your abdominal aortic aneurysm (AAA). It is important that you feel able to take an active role in your recovery.
This booklet gives you information on what to expect in hospital after your operation, advice about recovering from your surgery; and aims to prepare you for your recovery at home. It can be used together with information leaflets given to you before your operation.
We hope this information is helpful. If there is anything you do not understand, please ask any of your vascular team (the doctors, nurses and other healthcare professionals involved in your care).
Your Operation – Endovascular AAA repair
Fenestrated endovascular repair is a relatively new procedure that helps repair damage in segments of the aorta where it branches in to the blood vessels to your kidneys, small bowel and liver. When the endograft is positioned in the aorta, the fenestrations allow blood to flow to the kidneys and other organs by the use of smaller covered stents.
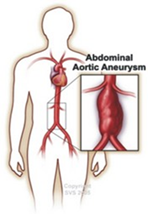
The aorta is the main artery which carries blood away from the heart through your abdomen and to the rest of your body. An aneurysm occurs when the walls of your arteries weaken, causing a swelling. An abdominal aneurysm is a swelling in the aorta, which is in your abdominal / tummy area.
What is an endovascular aneurysm repair (EVAR)?
EVAR is a minimally invasive ‘keyhole’ surgery to repair an aneurysm. It is performed through a small cut in your groin to gain access to the femoral arteries (blood vessels), rather than the large incision across your abdomen used in traditional surgery. It is performed in the Radiology (x-ray) Department by an interventional radiologist (a doctor who uses x-ray) and a vascular surgeon.
With EVAR, the aneurysm is repaired using a special stent graft (also known as an endograft). It is a small, fabric wrapped, flexible mesh tube used to ‘patch’ the ballooned section of blood vessel by inserting it through the small cut in the groin and placing it inside the artery, to strengthen it and prevent bursting.
What is a fenestrated or branched repair?
The Fenestrated device is a type of stent graft which is custom made for each individual patient. It has been chosen by your surgeon as the most suitable treatment option and has been customised to suit your specific anatomy. Although the same blood vessels and arteries are present in all of us, their exact position in the body, and in relation to each other, will vary from person to person. The Fenestrated device is commonly used to treat aneurysms that are not suitable for treatment with standard devices because of the specific anatomy of the patient.
This could be because:
- there is only a short distance between the top of the aneurysm and the renal arteries.
- the aneurysm involves the renal arteries and/or other arteries.
- the aneurysm also extends beyond the abdomen and into the chest.
For some patients with the above types of aneurysm, Fenestrated Endovascular Aneurysm Repair (FEVAR) is a treatment option which allows patients to avoid open surgery.
The advantage of FEVAR is that the area around the renal arteries and mesenteric arteries (which supply blood to the intestines) can be protected (or repaired if needed), while still allowing blood flow to these vessels. The Fenestrated device is designed with your doctor to specifically suit your blood vessels. A CT scan of your aorta is used to design a custom made Fenestrated which will fit your specific anatomy.
Once you have had your CT scan and your fitness test (CPX) the results will be discussed in a special complex aneurysm MDT. The fitness /CPX test involves you peddling on a stationary bicycle or using an arm crank whilst having your heart and lungs monitored by a specialist vascular anaethetist. The anaethetist will present your results at the subsequent MDT meeting.
What happens during the procedure?
The procedure is performed by an interventional radiologist and a vascular surgeon, using x-rays to guide medical instruments inside your arteries. In the procedure room, in the x ray department, you will be asked to lie on your back on an x-ray table. Monitoring equipment will be attached to you to measure your blood pressure and heart rate. A small tube (cannula) will be put into a vein in your arm for monitoring and to give you fluids.
You will have a general anaesthetic where you are asleep during
the whole procedure. You will have a tube (catheter) inserted into your bladder. A small incision will be made in each side of your groin.
For some branched endograft repairs it is necessary to also make a small cut in the left upper arm (axillary) area. A short tube, called a sheath, will then be placed into the artery to keep it open while a thin, flexible tube called a catheter is inserted into the femoral artery and directed to the aneurysm. Contrast (dye) is injected into the catheter and will show up on the x-ray monitor. A metallic spring with a cover (stent graft) that is compressed into a small diameter is passed through the catheter. The stent graft is advanced to the aneurysm, and then opened, creating new walls in the blood vessel through which blood flows. When the stent graft is deployed (opened) it seals the aneurysm.
What happens after the procedure?
You will be taken to the recovery room where you will need to stay flat in bed. You will be closely monitored by nurses who will periodically check your blood pressure, pulse and oxygen levels. You may still have a drip, a catheter and oxygen initially which are removed usually at day 1 post-operatively.
When your condition is stable and you are well enough to be transferred, you will be taken back to the ward. You will rest in bed overnight and you will be able to eat and drink normally.
The following morning we will do some blood tests and encourage you to walk around the ward. Any cannulas or lines used to administer medications and pain relief that you have will be removed.
You can expect to be allowed home two days after surgery. We will change your dressings the morning you leave hospital.
Your early recovery on the ward
Most patients will return to the ward after their operation. You may still have a drip, a catheter and oxygen initially, which are removed over 1-2 days.
Pain
The incisions (cuts) in your groins are likely to be uncomfortable at first. The nurses will monitor your level of pain and initially you will be given painkillers by a machine that you control yourself. Once you are eating and drinking, you will be able to take painkilling tablets by mouth. The pain will slowly improve but you may get twinges and aches for a few weeks.
Eating and drinking
Usually on the morning after your operation you will be able to eat breakfast and a light diet. Or if you feel like some supper on the day of your operation you may have it .It is normal to lose your appetite after surgery; as a result of this you may lose a little weight.
If needed, you can be seen by a dietitian, who might recommend that you take supplementary drinks in order to support your recovery.
Your wound
Your wound will be red at first but will gradually fade over six months or more. You can wash normally with mild soap and water when you have a bath or shower.
If your wounds become red, sore or there is oozing please let your GP know, as this could be a sign of an infection. Protecting your scar from exposure to sunlight during the first year after having surgery will prevent the scar becoming darker. Occasionally clips will be used to close your wound which will be removed 2 weeks after the operation by your practice nurses. Bleeding or bruising can occur under the skin where the catheter was inserted in the groin. This is known as a haematoma and can be common, and can take one/two weeks to disappear.
Moving around
On day one you will be encouraged to mobilize around the ward, by day 2 you should be finding it easier to walk around the ward area, and should resume gentle activity and get back to normal as and when you see fit.
Moving around will not cause any damage to the graft, or to your wound, and will help your recovery. If needed, a physiotherapist will give you individual assistance and instructions to help you regain your normal mobility.
Medication
Most people will be sent home on a small dose of aspirin to ensure the blood is less sticky and a statin to reduce your cholesterol levels. If you are unable to take aspirin an alternative drug may be prescribed. Any blood pressure tablets will be reviewed. You might already be on these tablets. When you go home you should continue with all your usual medications these will be reviewed by the doctors.
If you are taking Metformin, this should be withheld for 48 hours after the procedure and then continue as usual.
Preparing for discharge
Most patients go home about day 2 or 3 after their surgery, although this maybe longer if complications occur.
Preparing for home should start before your operation. It is a good idea to have someone to help look after you for a while, or some patients choose to live with a member of their family for a short time. Think about the tasks, or activities you do, which may be difficult especially if you have a caring role for someone else. Stocking up on frozen or tinned items means you don't need to go shopping immediately.
If there are any complications with your recovery, you may need to stay in hospital a little longer.
Recovery at home
Recovery times vary, and it can take couple of weeks to feel ‘back to normal’, and can depend on your health and activity before surgery.
Sleeping and feeling tired
It is normal to feel tired for at least 4 weeks after your operation. You may feel low in spirits. You might need a short sleep in the afternoon for a few weeks, as you gradually increase your level of activity. It is good for you and your family to be aware of this.
Diet and appetite
It can take a few weeks for your appetite and diet to return to normal and to regain any weight you may have lost in hospital. Try taking smaller regular meals. You may find your bowel motions take time to become more regular again.
Mobility, hobbies and activity - start slowly!
It can take several weeks to make a full recovery. During this time, you should not lift heavy objects, or undertake strenuous activities or sports such as golf. Taking regular exercise such as a short walk combined with rest is recommended for the first few weeks which you can gradually increase. Taking on light household chores, and walking around your house is a good starting point.
Working
When to return to work will depend on the type of job you do. Most people need to wait 4-6 weeks before returning to work and may work shorter hours for a few weeks and build back up to their normal hours.
Sex
You can resume your sex life when you feel comfortable. Rarely, men can have problems sustaining an erection after this operation as the nerve supply may be disturbed. This affects approximately 10% of men. It is not known what effect, if any, AAA repair has on a woman’s sex life. If you experience problems, your GP or consultant will be able to refer you to a specialist.
Driving
For safety and insurance reasons patients are unable to drive for 4 weeks after their operation. If you are in doubt, you should check with your GP and insurance company.
Exercise programme
Here are some tips for planning your exercise at home but your ability to exercise will depend on your fitness before surgery.
Week 1 Walk gently around the house and garden. Take an afternoon nap if needed.
Week 2 Take a daily 5-7 minute small walk around your house and garden. Take an afternoon nap, if needed.
Week 3 Take a short 7-15 minute walk in the morning and afternoon. Take a nap in the afternoon if needed.
Week 4 Take a 15-20 minute walk, twice a day if possible. Some days you might need a nap.
Complications and what to look out for:
If you think that there is something wrong with your wound once you get home, you should contact your GP or the ward from which you were discharged.
The things to keep a look out for to tell the vascular team are:
- pain in your legs when walking
- a redness or swelling in the wound
- continued poor appetite, upset bowel movements.
Outpatient follow-up
After a fenestrated endovascular repair, you will be sent an appointment to have a CT scan at 30 days post-operatively and see your consultant 2 weeks after that to review your scan and your recovery progress.
You will then need to have an ultrasound scan at 6 months then at a year, and continue repeat ultrasound scans on a yearly basis, to make sure that the stent is in place and there are no signs of leaking. You will also have your blood taken at these intervals to check your renal function.
These appointments will be sent in the post to you, and the results will be sent to your consultant and if the scan and bloods are normal the consultant may not need to see you.
Medications and Surgery
Angiotensin-converting enzyme inhibitors or ACE inhibitors (e.g., Enalapril, Lisinopril or Ramipril) should not be taken on the day of surgery.
Angiotensin II receptor blockers or ARBs (e.g., Candesartan, Losartan or Valsartan) should not be taken on the day of surgery.
Clopidogrel should be stopped 7 days pre-operatively for vascular operations except for all carotid endarterectomies or unless directed by your consultant. If you have had a stent inserted into your heart in the last 12 months, please inform your consultant and this will be discussed with a cardiologist as to the decision of when to stop your Clopidogrel.
Warfarin. If you are currently taking Warfarin this will be discussed with you by your consultant, regarding if this needs to be stopped and if you need a covering anticoagulant.
Direct oral anticoagulants or DOAC (e.g., Rivaroxiban, Apixaban or Dabigatran) . This should be stopped at least 48hrs prior to the procedure if high risk of bleeding. If your kidney function is abnormal, this may need to be discontinued for a longer time period prior to surgery. If you take Ticagrelor it will need to be discontinued for 5 days.
Your consultant will advise about this.
Following the procedure, the DOAC will be restarted after 24-72 hours at the discretion of your consultant. You will be started on an anticoagulation injection (e.g., Dalteparin) to help prevent blood clots on the evening of the procedure and daily until the DOAC is restarted. This will be stopped once the DOAC has been restarted.
T.E.D Anti-embolism stockings should never be given for arterial patients unless specifically directed by the consultant, if you are asked to apply a pair please can you question this with a member of the vascular team.
Along with toiletries, night clothes, etc., the vascular team actively encourages all our patients to bring in day clothes to wear on the ward whilst an inpatient and to have ready for discharge.
Contact Details
Secretaries at Frimley Park
Mr D J Gerrard, Mr Chong, Mr Chaudary 03006132141
Mr K Jones, Mr Cleanthis, Miss Moore 03006134291
Lt Col Sharrock, Mr Ali, Mr Dastur 03006132487
North Hants Hospital Basingstoke Secretary
Wexham Park Hospital Secretary
Vascular Specialist Nurses
Claire Martin Lead Vascular CNS - FPH 0300 6136302
Tracey Craig Vascular CNS - FPH
Andrea Croucher Vascular CNS - FPH
Pabita Limbu Vascular CNS - FPH
Kirstie Lane Vascular CNS - WPH 07770702053
Nessa Cababa Vascular CNS - ASPH 07522618600
Contact us
If you have any queries relating to this information, please contact the Vascular surgery service.
About this information
Service:
Vascular surgery
Reference:
Y/041
Approval date:
7 March 2024
Review date:
1 March 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.