Advice after your nerve block for surgery
On this page…
Introduction
The aim of this leaflet is to give you a general understanding of what happens before and after your operation. It is designed to help you to prepare for your operation and after care once you go home.
Your Shoulder
-
-
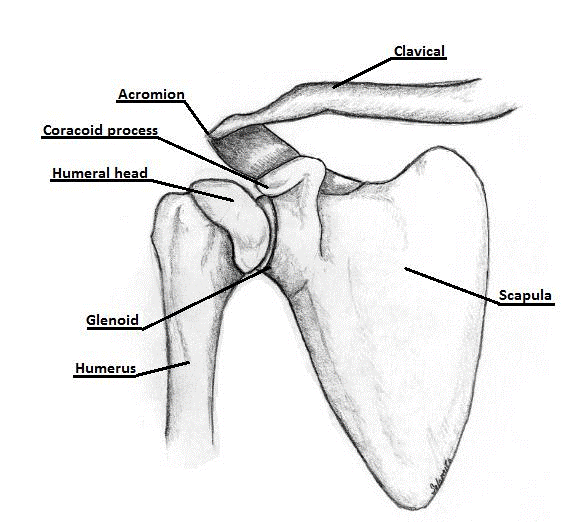
The ball is on the bone of the upper arm (the humerus) and the socket on the shoulder blade (the scapula).
-
The joint is supported by the rotator cuff muscles.
-
These muscles may become damaged after trauma or with age.
Shoulder Replacements
There are different types of shoulder replacement surgery. Your consultant will have assessed your shoulder and discussed the most appropriate surgery for you.
Copeland shoulder
Resurfacing of the humeral head (the ‘ball’). This is a ‘hemi-arthroplasty’ as the glenoid ‘socket’ is not replaced.
Total Shoulder Replacement
This involves the replacement of both the ball and socket joint. It is also known as an Anatomical Shoulder replacement.
Reverse Total Shoulder Replacement
This involves creating a socket on the top of the humerus bone and fitting a ball on to your socket. This type of shoulder replacement is used if the rotator cuff tendons around your shoulder are torn or non-functional because it relies on different muscles to move the arm or if there is significant bone loss due to the arthritis.

Figure 1: a) Anatomic total shoulder replacement - metal 'stemless' humeral head and plastic socket (therefore not seen easily on Xray)(left) b) Reverse total shoulder replacement (right)
What are the alternatives?
You may have tried various non-surgical courses of treatment such as painkillers, injections, exercise, and physiotherapy to help improve your pain and function.
However, if these have failed and your symptoms are intrusive, then shoulder replacement surgery is generally recommended.
What happens before your admission to hospital?
You will be contacted by the pre-operative assessment clinic to assess your fitness for surgery. You will be given information regarding your surgery, and you will be able to ask questions. You will also be contacted by the therapy team to discuss how you will manage your daily activities following your surgery. This may be a face to face or a telephone appointment.
Coming into hospital
You will be admitted to hospital on the day of your surgery. Admissions times vary but are typically 7am or 12pm. You will not be allowed to eat anything for 6 hours prior to your surgery. You can drink tea/coffee with a small amount of milk up to 2 hours before your surgery. Clear fluid (water/black tea/coffee) is allowed until you are called to theatre. You may also receive a carbohydrate drink 2 hours prior to your surgery.
You will normally be discharged home within 24 hours of your surgery. In some circumstances, this may be on the same day and would be discussed with you prior to admission. There are many advantages to being in your own environment, reducing the risk of complications and being in control of your own recovery.
You will need to arrange for someone (e.g. a family member or a friend) to bring you to and from the hospital as you will not be able to drive home after your operation.
You will only be discharged home if it is medically safe to do so, you have someone at home with you and can manage safely. If there are any concerns, you will stay in hospital overnight and go home the following morning.
After your operation
The operation takes approximately one to two hours, which includes anaesthetic time.
You will wake up in the recovery room of the theatre, where you will remain until you are awake. You will be wearing a sling.
Pain relief
It is important to take your painkillers as prescribed to keep pain to a minimum. This will also enable you to do your exercises more easily in the first few days after your operation. Ice can be helpful to reduce pain/swelling. Protect your dressings from getting wet with a plastic bag. Wrap a bag of ice/frozen peas in a damp towel and apply for 10-15 minutes. This can be repeated every 3-4 hours.
Wound care
Following your operation, you will usually have a wound, at the front of the shoulder and these will be covered with a dressing. Your wounds need to be kept clean and dry until they have healed (usually about 10 days). The nursing staff will provide you with more information about wound care on discharge. At 2 weeks after your operation you will attend a nurse physio/led clinic for your wound to be checked.
Getting moving after the operation
You will be assessed by the Physiotherapy team after your operation. You will be shown how to take your sling on and off, along with some gentle arms exercises. They will also ensure you are able to mobilise safely and will complete a stair assessment if needed. Once you are discharged from hospital, you will be referred for outpatient Physiotherapy which will start in accordance with your surgeons’ protocol.
Activities of Daily living
You may be assessed by an Occupational therapist after your surgery to discuss how you will manage your daily activities whilst wearing the sling. You will be one handed for a period of time and the following advice gives some tips on how to manage.
Washing and Dressing
You will need to wash and dress your body using your un-operated arm. Depending on your restrictions you may be provided with a sling for showering. Showering with a non-slip mat in place is advised as opposed to taking a bath to protect the wound and to avoid weight bearing on your operated arm. Your wound dressing is water resistant; however, you should avoid direct exposure to water when showering. Please be advised that your balance may be affected while wearing a sling and therefore consider safety aspects when stepping in/out of the bath/shower or on uneven ground. You could purchase a bath board for over the bath. Always support your arm in your sling, on your lap or on a surface in front of you.
You will require loose clothes, preferably ones that button down the front. Avoid clothing with small buttons, hooks and zips. Ladies may find a bra uncomfortable and may prefer to wear a strapless or front-fastening bra. Consider slip-on, easy fitting shoes.
You will usually be allowed to wear your sling over clothes but will need to check this with the team. Always dress your operated arm first and undress it last. You should sit when dressing, with your operated arm resting on your lap.
Dressing Procedure in a Sling
1. 


- Sit on the bed and place a pillow(s) under your arm so it is rested in the sling position.
- Undo the buckle and Velcro fastenings at the elbow and wrist. This will release the shoulder strap. You may need assistance.
- Gently slide out the sling from underneath your forearm by pushing down into the pillows. Keep the operated shoulder as still as possible.
- Thread the sleeve onto your operated arm and take the garment as far up to the shoulder as possible. Keep the operated shoulder as still as possible. You will then be able to put your non operated arm into the sleeve, bringing the garment up and around your shoulders to do the clothing up.
- Replace the sling by gently sliding it under your forearm. Replace the buckle and Velcro fastenings. You may need assistance.
- To fit sling reverse steps 3 to 1.
Sleeping
Avoid lying on your operated arm initially. Lying on your back may be the most comfortable position. A pillow placed behind the operated arm may be advised to prevent the arm from falling backwards. Your therapist will advise you.
Sleep is important in your recovery, and can be a bit of a challenge after an operation. Here are some tips that may help:
Take your painkillers just before bed. You may find the following sleeping positions helpful. Use pillows to help support your operated arm as shown below.

Standing from Chairs, Toilets and Beds
It can be quite difficult to stand from low furniture. If you feel that you will struggle with this post operatively raising the height of furniture can be helpful, e.g., using an extra cushion, raised toilet seat, chair or bed blocks.
Domestic Tasks
It is advisable to cook extra meals and stock up with freezer food. Use ready prepared meals or items that need little preparation, e.g., pre-chopped vegetables. You will need to do kitchen tasks using your un-operated arm.
There is equipment available that can help with food preparation, for example easy grip jar openers, pizza cutters. You will not be able to lift large or heavy dishes on or off the hob or in and out of the microwave. We suggest you prepare food in small dishes that are easy to hold and carry in one hand. If you use a walking aid, we suggest you sit in your kitchen to eat and drink.
You should avoid heavy household duties that may put undue stress on your shoulder until approximately 12 weeks post op or when advised by your physiotherapist.
If you live alone, it is advisable to stay with someone or arrange for someone to come in and help you with household tasks, shopping and looking after pets. Social services will not provide support with domestic tasks.
General Guidelines
Pain
A nerve block is used during the operation which means that immediately after the operation the shoulder and arm may feel numb. This may last up to 24 hours. After this the shoulder will feel sore and you will be given painkillers to help this whilst in hospital. These can be continued after you are discharged home. Ice packs may also help reduce pain. Wrap frozen peas or crushed ice in a damp, cold cloth and place on the shoulder for up to 15 minutes. It may take several months for the pain to fully settle but, in the long-term, your level of pain should be significantly reduced compared to how it was before your operation. If you are struggling with pain post operatively please get in touch with the nurse care team on 0300 614 4130 / 0300 614 4131
What is a nerve block?
Your anaesthetist will inject a local anaesthetic around the nerves at the side of your neck. This blocks the pain signals that come in the nerves from your shoulder (just like the dentist does when he works on your teeth) and thus limits the pain you would feel when you wake up.
Will it hurt?
If the nerve block is done after you go to sleep you will feel no pain for several hours after your surgery. Sometimes, however, the anaesthetist prefers to do the nerve block just before you go to sleep. In this case there is some mild discomfort only, and the anaesthetic will cause your shoulder to “twitch” involuntarily for a few seconds. This indicates that the local anaesthesia is in the correct place.
Are there risks?
In general, the risks of nerve blocks are very low. The arm will feel numb or there will be no feeling in it while the block is working. You may have tingling in your fingers or even a drooping of the eye lid on the same side. This is because all these nerves originate near to the shoulder nerves in the neck and the local anaesthetic may spread to involve them. All these side effects will wear off when the block wears off.
Are there any long-term risks?
The risks of any long-term numbness or weakness of the arm or diaphragm are very small. Permanent nerve injury risk from an interscalene nerve block is approximately 1 in 10,000.
What happens when the block wears off?
As the block wears off, you will start to feel some discomfort in your shoulder. You will be closely monitored by the nursing staff on the ward but do let them know if you are not comfortable. We recommend you take the painkillers offered to you after your surgery before your block wears off, so you have painkillers ‘on board’ as the block fades. This will make your experience more comfortable.
What happens when I go home?
You will be contacted by the Arthroplasty Nurse or a member of the ward team the day after your discharge to see how you are managing at home.
You will also be given the ward telephone numbers to contact 24/7 should you have any questions or concerns.
Your wound will be covered with a waterproof dressing and should not be changed or disturbed until your stitches are removed at two weeks. It is normal to see blood-stained fluid on the dressing.
Follow-up Appointment
You will have a follow up appointment at two weeks post-surgery. This appointment is a joint therapy/nurse led review. Your wound will be reviewed, and the therapy team will assess your shoulder and may progress some of your exercises
Outpatient Physiotherapy will start in line with your Surgeons post-operative protocol.
You will see your Surgeon 6-12 weeks post-surgery.
Driving
Depending on the type of surgery you have, you can return to driving from six weeks. You cannot drive whilst wearing a sling. You must be confident and competent to control the steering wheel (and gearstick) for routine and emergency manoeuvres.
Return to work
If you have a desk based/sedentary job, you may return to work from six weeks. If you have a physical/manual job, you will be guided by your Consultant.
Leisure activities
- You can begin swimming from three months.
- You can return to golf from three months.
- You should avoid heavy lifting for six months.
For guidance on any other activities, you should speak with your physiotherapist and Consultant.
What are the risks and possible complications?
Uncommon (1-2%)
Infection: Infection around a new joint is a serious complication. It is therefore important that you do not have any infections prior to surgery, for example, skin, chest or urinary tract infection. Should you have an infection prior to your surgery, please inform the pre-assessment staff.
Wound healing problems: The scar will be over the front of your shoulder. Dissolvable sutures are typically used. It is rare for the wound not to heal nicely, but occasionally this may occur.
Anaesthetic risks: Modern surgical practice is very safe, but shoulder replacement requires a general anaesthetic and normally a nerve block (to numb the whole arm for 18-24hrs to reduce peri-operative pain). There are small risks associated with anaesthetics and these risks are increased for those patients with significant pre-existing medical problems.
Rare (less than 1%)
Bleeding: This is usually small. It is rare to require a blood transfusion. The current transfusion rate in our unit is less than 1%. You may see bruising around the shoulder, the front of your chest and down to the elbow. This will subside and should not require any treatment.
Nerve injury: Whilst rare, injury to the nerves around the shoulder can occur during surgery. If nerve injury does occur, it may cause weakness of the shoulder or arm muscles. Normally, nerve injury is the result of a stretch to the nerves and will recover with time; but permanent injury can (very rarely) occur.
Instability: This is very rare and may require further surgical treatment if it is an ongoing problem.
Fracture or implant failure: These are rare and will be dealt with during the operation if they occur. Later fracture around a shoulder implant can happen following a fall, and this may sometimes require surgery to fix the fracture and/or revise the implant.
Loosening and wear: Over time the replacement bearing may wear and become loose and/or painful. This may happen over a period of 10-20 years following surgery and sometimes requires revision surgery.
Post-op blood clots (DVT): The risk is very low after shoulder replacement (less than 1%) and is reduced as much as possible by early mobilisation, compression device pumps, exercises and medication to thin the blood.
Useful Contacts
Heatherwood Hospital:
- Orthopaedic pre assessment 0300 614 7778 / 0300 614 7147
- Arthroplasty Nurse Heatherwood 07789927177
- Nurses Station Treetops Heatherwood 0300 614 4175
- Physio/OT Office Treetops Heatherwood 0300 614 4178
Frimley Park Hospital:
- Frimley Park Physiotherapy 07570 974390
- S2 Elective Ward Frimley 0300 613 3781 / 0300 613 3783
- Elective Helpline Frimley 0300 613 2556
Wexham Park Hospital:
- Ward 1 Wexham Park 0300 615 3010 / 0300615 3012
- Outpatient Physio Wexham 0300 615 3501 / 0300615 3500
- Wexham Park Physiotherapy 07717 199851
Contact us
If you have any queries relating to this information, please contact the Orthopaedics service.
About this information
Service:
Orthopaedics
Reference:
N/070
Approval date:
13 May 2025
Review date:
13 May 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.