Advice after your nerve block for surgery
On this page…
Introduction
To understand the reasons why some individuals suffer with nasal blockage and sinusitis, it is necessary to consider the anatomy and physiology of the nose and sinuses.
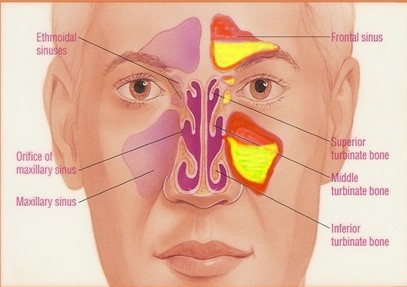
The inside of the nose is separated into 2 cavities by the nasal septum which should be in the midline. Connected to the nose by a series of narrow clefts are 4 pairs of sinuses which are air filled cavities in the skull.
The 4 paired sinuses are the maxillary, frontal, ethmoid and sphenoid. All of these sinuses and the inside of the nose have a very specific lining or mucosa. It consists of cells with cilia, microscopic hair like structures which vibrate in coordinated fashion to transport mucous and any other debris from the sinuses into the nose and subsequently into the throat. From here, the mucous is swallowed. Interspersed with the cells which have cilia are other cells which produce the mucous.
Therefore, mucous is continuously produced in all individuals and transported by this process of ‘mucociliary transport’ from the sinuses and nose into the throat. In healthy individuals this occurs without the individual knowing that this is happening.
The maxillary, frontal and anterior ethmoid sinuses all drain into the nose via the same series of clefts and channels, and enter the nose on either side under a structure called the middle turbinate. In fact, there are 3 turbinates on the outer wall of both sides of the interior of the nose. Their function is to humidify air and direct it to the back of the nose.
The area under the middle turbinate where these sinuses drain has been termed the ‘middle meatus’ and this area combined with the drainage clefts is called the ‘ostiomeatal complex’.
Blockage in this ostiomeatal complex may occur secondary to mechanical factors, and also swelling or oedema of the mucosa. More commonly a combination of several factors blocks this specific area. When this occurs the normal mucous transport system is affected and mucous becomes stuck in the sinuses.
This stagnant mucous becomes an excellent culture medium for a variety of pathogens including bacteria. If bacteria multiply in the blocked sinuses then sinusitis occurs. Usually this will settle with antibiotic therapy, but sometimes the infection can last many weeks and becomes chronic.
In addition, occasionally infection can spread to the bone surrounding the sinuses, and from here extend to the eye and brain. Sinusitis can be a serious infection.
It is important to consider the mechanical factors and the mucosal factors which may contribute to sinusitis. In addition to causing nasal blockage, a severe deviation of the nasal septum can predispose patients to sinusitis.
There are also certain anatomical arrangements of the clefts from the sinuses to the nose which can also make sinusitis more likely. Perhaps the most important consideration should be given to the causes of swelling of the nasal and sinus mucosa, as some of these are treatable with medicines and other measures. They also frequently contribute to nasal blockage.
The commonest cause of mucosal swelling leading to blockage and sinusitis is acute viral rhinitis or the common cold. As patients know only too well, sinusitis can often follow a nasty cold. Allergic rhinitis or inflammation inside the nose as a result of allergy can also cause blockage and sinusitis. In patients with sinus problems, it is important to exclude allergy as a contributory factor.
Patients are often tested for the common allergens that may be inhaled into the nose. These include pollens from cats, dogs and other domestic pets. If allergy if a factor it should be treated accordingly.
The next issues to consider in terms of mucosal inflammation and swelling are atmospheric pollution and smoking, both of which can contribute to nasal blockage and sinusitis. There are of course other causes of sinusitis, including dental problems, but the commonest causes all relate to blockage of the ostiomeatal complex and interference with mucocillary clearance.
Usually this is due to some form of inflammation leading to swelling or oedema. In certain cases the oedema is of such a magnitude, that within the narrow drainage clefts of the sinuses, nasal polyps form. These can extend into the nose and contribute to nasal blockage and sinusitis.
As you can see, nasal blockage and sinusitis have many different causes. The problem is multifactorial and therefore treatment must be directed at all the various elements discussed.
Treatment options include antibiotics to fight infection, nasal steroid sprays and drops to treat nasal inflammation and polyps, other anti-allergy measures, and sometimes nasal and sinus surgery. Options range from straightening the nasal septum to widening the drainage clefts from the sinuses into the nose; often in combination with removal of nasal polyps. This sort of surgery uses a key-hole approach.
In summary, nasal blockage and sinusitis occur for many different reasons. As such a number of different treatments may be required.
Contact us
If you have any queries relating to this information, please contact the Ear or nose and throat (ENT) service.
About this information
Service:
Ear, nose and throat (ENT)
Reference:
G/021
Approval date:
23 February 2026
Review date:
1 February 2029
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.