Advice after your nerve block for surgery
On this page…
Introduction
This information tells you about treatment of abdominal aortic aneurysms.
Repair of an AAA is a surgical procedure that is usually carried out when the risk of an AAA rupturing (bursting) is higher than the risk of an operation. Your aneurysm may have reached a size at which surgery is considered the best option for you. This leaflet provides information about your options for treatment. It is not meant to be a substitute for discussion with your Vascular Specialist Team.
What is the aorta?
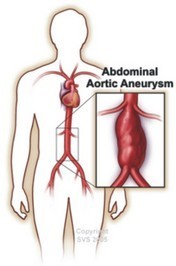
The aorta is the largest artery (blood vessel) in the body. It carries blood from the heart and descends through the chest and the abdomen. Many arteries come off the aorta to supply blood to all parts of the body. At about the level of the pelvis the aorta divides into two iliac arteries, one going to each leg.
What is an aneurysm and an abdominal aortic aneurysm?
An aneurysm occurs when the wall of a blood vessel is weakened and balloons out. In the aorta this ballooning makes the wall weaker and more likely to burst. Aneurysms can occur in any artery, but they most commonly occur in the section of the aorta that passes through the abdomen. These are known as abdominal aortic aneurysms (AAA).
What causes an AAA?
The exact reason why an aneurysm forms in the aorta in most cases is not clear. Aneurysms can affect people of any age and both sexes.
However, they are most common in men, people with high blood pressure (hypertension) and those over the age of 65.
The wall of the aorta normally has layers of supporting tissues. As people age, they may lose some of this tissue. This is thought to explain why aneurysms are more common in older people.
Your genetic make-up plays a part as you have a much higher chance of developing an AAA if one of your immediate relatives (parent, brother or sister) has or had one.
Certain other 'risk factors' increase the chance of getting an aneurysm. These include: smoking, high blood pressure, high cholesterol, emphysema and obesity.
How are aneurysms discovered?
The majority of AAAs cause no symptoms and are discovered by chance. A routine examination by a doctor or an x-ray or scan performed for some other reason may pick up the presence of an aneurysm.
Alternatively, some patients notice an abnormal pulsation in their abdomen. As the aneurysm stretches it can also cause pain in your back or abdomen.
Nationally screening for AAAs has been introduced. This is performed using an ultrasound scan. The scan will tell you if there is an aneurysm present and exactly how large it is. It is performed in your 65th year.
A more detailed CT scan is sometimes done. This may be done if your doctor needs to know whether the aneurysm is affecting any of the arteries that come off the aorta. CT scans are also done by surgeons to help plan an operation.
If an aneurysm is suspected on clinical examination, or found on ultrasound, your GP will refer you to a Vascular Surgeon for advice.
What are the symptoms of an AAA?
Aneurysms generally take years to develop and it is rare for them to give symptoms during this time. If you do develop symptoms you may experience one or more of the following:
- A pulsing feeling in your abdomen, similar to a heartbeat.
- Pain in your abdomen or lower back.
What is the concern about an AAA?
The main concern is that the aneurysm might rupture (burst). The wall of the aneurysm is weaker than a normal artery wall and may not be able to withstand the pressure of blood inside. If it ruptures then internal bleeding occurs which is often fatal. Of course, most AAAs do not rupture - only a certain proportion.
What is the chance of an AAA rupturing?
The chance of rupture is very low for small AAAs. For aneurysms measuring less than 5.5cm in diameter the risk of rupture is less than 1 in 100 per year. As aneurysms get larger than 5.5cm, the risk of rupture increases and it is usually at this size that the option of surgery is considered. For any given size, rupture risk is increased in smokers, those with high blood pressure, and those with a family history of an AAA.
Each individual’s risk from their AAA and from surgery may be different, so any decision on treatment will be carefully considered by your vascular team and always discussed in detail with you and, when appropriate, your family.
If you experience sudden onset of new severe abdominal pain or back pain that is distinct from any back pain you may have had previously, you may be developing a leak from your AAA or at immediate risk of rupture.
If you experience any of these things please dial 999 for an ambulance and tell the ambulance control that you have an aortic aneurysm and need to go urgently to hospital.
Do not drive yourself to hospital.
Should everyone with an AAA have surgery?
The short answer is no. Surgical repair of an AAA is a major operation and carries risks. Research has shown that for people with aneurysms, measuring less than 5.5cms (about 2 inches), it is safer not to operate as the risks of having an operation are greater than the benefit.
Treatment Options for AAAs
Surgery is commonly advised if you develop an AAA larger than 5.5cm in maximum diameter (about 5 cm in women). For these larger aneurysms, the risk of rupture is usually higher than the risk of surgery. If you have a family history of ruptured aneurysm; surgery is also likely to be advised.
The two types of operation available to repair your AAA are Open Surgery or Endovascular Repair.
However, if your general state of health is poor, or if you have
certain other medical conditions, this may increase the risk if you have surgery. In some circumstances therefore the decision to operate may not be straightforward, and your surgeon may advise that you be medically managed if you are unfit for surgery.
What will happen after my outpatients’ appointment?
If you are being considered for treatment you may be asked to return to undergo tests of your fitness for surgery and the associated risks, along with a CT scan to examine your AAA more closely. You will be discussed in a meeting involving a surgeon, radiologist and anaesthetist to agree the best options in your case. Your specialist vascular surgeon and team will then give you a clear explanation and you will have full discussion involving your personal choice before a decision is made. Your best interests will always be taken into account and you are not obliged to undergo any treatment that you do not want.
Medical Treatment
If you are unfit for surgery at the current time, your doctor may wish to advise medical treatments aimed at keeping you healthy and reducing the risks of rupture of your AAA. These will include treating any high blood pressure and a high cholesterol and improving your fitness by treating any heart lung or kidney disease so that an operation may be performed at a later time. Patients with diabetes are less likely to have problems with surgery if their diabetic control is good.
Regular moderate exercise can also help keep your heart and lungs healthy.
If you are fit for surgery two types of operation may be performed.
Open Repair
The traditional operation involves cutting open your abdomen to replace the aneurysm with an artificial piece of artery (a graft). This is a major operation and carries some risk. However, it is successful in most cases and the long term outlook is good. The graft usually works well for the rest of your life.
Complications: The risk of a major complication is about 5 to 7% from an open operation.
Recovery: If your recovery is straightforward, you will be in hospital about 7 days. It is not unusual for patients to spend one or two nights on the high dependency or intensive care unit. You will be allowed to eat and drink once you are fully awake following surgery. You may not feel like eating immediately, but usually you will be eating normally within 3 days of your operation. The nurses will aim to getting you sitting up and walking as soon as possible.
Once you are well enough to return home, you will be discharged. At this stage, you may still need painkilling tablets. You may also notice that you tire easily. It is usual for it to take at least three months, and sometimes longer, to get back to your normal level of activity. During this phase of recovery, you should plan periods of rest into your day, gradually reducing them as you get stronger. The best way to recover is to gradually increase your level of physical activity over three months. You may resume normal sexual relations as soon as you as you feel comfortable.
Your wound should be dry and healed within 10 days. If you develop redness or swelling in the wound, you should see your doctor about this. You will be referred back to your surgeon if your doctor has any concerns.
Returning to work: There is no set time for returning to work but you may need to wait 6-12 weeks before you are able to work. You should ask your surgeon about this. If you drive for a living, especially HGVs, you will need to be fully recovered before returning to work (see section on driving below).
3. Endovascular Repair
This involves inserting a graft within the aneurysm through small groin incisions using X-rays to guide the graft into place. The advantage of this type of repair is that there is no abdominal surgery. This technique is therefore safer than the traditional operation, and you need to spend less time in hospital.
A disadvantage is that some patients have to undergo a further operation at a later stage to refine the initial procedure. Not every patient or every aneurysm is suitable for this. In particular, aneurysms arising close to or above the kidneys are more difficult to treat in this way. You will be assessed with a scan to determine if your aneurysm can be treated by endovascular repair. If suitable you will be offered a choice of type of repair by your surgeon. If this cannot be undertaken at your local hospital, you may need to travel to a centre that can perform endovascular repair.
Complications: The risk of a major complication is lower for endovascular repair, as the operation does not interfere with the circulation as much as open surgery. Risk of death is 1 to 2%.
Occasionally following endovascular repair the aneurysm sac may continue to increase in size. This is known as an endoleak. Depending on the size or nature of the endoleak further intervention may be required. You will continue to have monitoring of your aneurysm indefinitely following your EVAR repair.
Recovery: After uncomplicated endovascular repair, most patients return to the hospital ward for one to two days. You should be able to eat and drink normally once fully awake following your aneurysm repair. The nurses will aim to getting you sitting up and walking as soon as possible.
Once you are up and about, you should be able to leave hospital, but may need painkilling tablets for up to a week. Discussions with patients who have undergone endovascular repair suggest that it can be normal to make a full recovery in about 2 weeks, however some people take longer and can tire and take several months to return to the health state they had prior to the operation. During this time, you should gradually build up your level of activity back to normal. You may resume normal sexual relations as soon as you as you feel comfortable.
Return to work: Most people who are treated with endovascular repair can return to work within a month after having surgery. If you drive for a living, please read the section on driving toward the end of this information sheet.
Is surgery successful?
If aneurysms are successfully repaired, this prevents them blocking or bursting and there is a very high likelihood that you will return to a normal life. Full recovery takes between 3 and 6 months after open surgery and 2 to 4 weeks after endovascular repair. The speed of recovery will also be affected by your age and general fitness.
What are the risks of surgery?
As with any major operation general complications can occur including infection in the wound, chest infections or diarrhoea.
There is a small risk of you having a medical complication such as:
- Heart attack
- Stroke
- Kidney failure
- Chest problem
- Loss of circulation in the legs or bowel
- Infection in the graft used to replace your aorta
- Death
Up to 1 in 10 men may have difficulty sustaining an erection following surgery due to injury to nerves which lie on the front of the aorta. It is also recognized to occur following endovascular repair. If you have problems with this, please tell your doctor, as there are treatments that may help.
Deep vein thrombosis (DVT) is a recognised risk and most patients will have treatment during their stay in hospital to prevent this. If you do develop a DVT, then you may require extra treatment for this and this may prolong your stay in hospital.
If your risk of a major complication is higher than this, usually because you already have a serious medical problem, your surgeon will discuss this with you. It is important to remember that your surgeon will only recommend treatment for your aneurysm if he or she believes that the risk of the aneurysm bursting is higher than the threat posed by the operation. Your surgeon will be able to tell you the success rate for this operation in his/her unit.
Consent to store your personal information
Vascular surgeons record information about surgical interventions, including AAA repairs, on the National Vascular Registry (NVR). This is a secure database that is used to help monitor and improve vascular services throughout the country. Therefore, you (or your nearest relative) may be asked to give permission for your personal information to be stored on the NVR. Although the database is a national system, strict data governance means personal details on the NVR can only be accessed by staff involved directly in an individual's treatment. Patient information is confidential and is not passed on to third parties other than healthcare professionals directly involved in an individual's care. You need to let your vascular surgeon if you are unhappy for them to store your personal information on the NVR.
What can I do to help myself?
Smoking. If you are a smoker the single most important thing you can do to help yourself is to give up smoking. Stopping smoking will also help to protect all of your arteries making it less likely that you will suffer from heart attacks or strokes. Giving up is not easy but there is a smoking cessation service and support groups that can help. Your vascular specialist nurse or GP practice nurse can advise you about these.
Inactivity. Gentle exercise such as walking and cycling are recommended to help to improve your overall level of fitness. Exercise helps your body to produce healthy cholesterol and this helps to protect your arteries against bad cholesterol.
High blood pressure. High blood pressure is a known risk factor for rupture of aneurysms. It is very important that you have your blood pressure checked regularly, at least every 6 months. If you have been prescribed medication for high blood pressure you must make sure that you take it according to the instructions given.
Diabetes. If you have diabetes it is important that your blood sugar levels are well controlled.
High blood cholesterol levels (fatty substance) in your blood. You should eat a healthy balanced diet and try to reduce any excess weight. It is important to reduce the level of cholesterol in your blood: you will be given advice on how to do this. Your vascular nurse can refer you to a dietician if needed.
You may be prescribed a statin drug to lower your cholesterol level and low-dose aspirin to help prevent blood clots from forming.
Driving with an AAA
Bus, coach and lorry licence
You must tell the DVLA if you have aneurysm of any size.
Car or motorcycle licence
You must tell the DVLA if the abdominal aortic aneurysm is greater than 6 cm.
Flying Advice
There is a theoretical increase in the risk of your aneurysm growing if you are a frequent flyer. Whilst we have no objections to you flying when your aneurysm is under 5cm once it reaches 5cm you may fit it difficult obtaining travel insurance.
Research
The Vascular Team at Frimley Health are actively involved in vascular research projects. You may be asked to participate in a research project as a patient if you are felt to be suitable.
Your data may also be used for the National Vascular Registry if you require certain operations or procedures.
Should you have concerns about your personal data and its use, please discuss with your clinician involved in your care. Data is entered automatically to the national database unless you notify us of your dissent.
Any Questions?
If you have any questions about this procedure or treatment, please make a note of them (to ensure you do not forget them) and ask them at your next appointment. Alternatively you may contact your Consultant via his/her secretary.
Contact Details
Secretaries at Frimley Park:
Mr Gerrard, Mr Chong, Mr Chaudary 03006132141
Mr Jones, Mr Cleanthis, Miss Moore 03006134291
Lt Col Sharrock, Mr Ali, Mr Dastur 03006132487
North Hants Hospital Basingstoke Secretary
Wexham Park Hospital Secretary
Vascular Specialist Nurses:
Claire Martin Lead Vascular CNS - FPH 0300 6136302
Tracey Craig Vascular CNS - FPH
Andrea Croucher Vascular CNS - FPH
Pabita Limbu Vascular CNS - FPH
Kirstie lane Vascular CNS - WPH 07770 702053
Nessa Cababa Vascular CNS - ASPH 07522 618600
Contact us
If you have any queries relating to this information, please contact the Vascular surgery service.
About this information
Service:
Vascular surgery
Reference:
Y/051
Approval date:
7 March 2024
Review date:
1 March 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.