Advice after your nerve block for surgery
On this page…
Introduction
Peripheral Arterial Disease (PAD) gives rise to narrowing or blockages in the blood vessels which limit blood flow to the legs. This can cause symptoms such as muscle pain, and tissue damage as the affected regions are deprived of blood and oxygen.
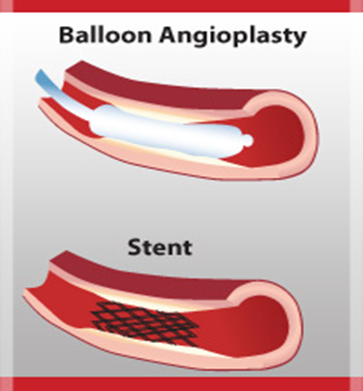
Angioplasty or stenting is a procedure used to treat the arterial narrowing or blockage. This uses either a balloon to stretch the artery (angioplasty) or metal scaffold to hold the artery open (stent). These procedures improve blood flow helping to relieve your leg symptoms. If you have been referred for this procedure, you will have seen a vascular surgeon for the symptoms caused by PAD.
The following information will help explain the process of angioplasty and stenting.
What does the procedure involve?
The procedure is performed in the Vascular X-ray Department by a Consultant Radiologist (x-ray doctor). Local anaesthetic is used to numb the skin and a small tube is placed in the artery in the groin, this is the only uncomfortable part of the procedure.
In some cases it may not be possible to use the groin artery and an alternative artery in the elbow is used.
A series of pictures are then taken of the arteries by injecting x-ray dye (contrast) into the tube. The contrast will give you a warm feeling each time it is injected and may give you the feeling of passing water. It may also give you a metallic taste in your mouth. Do not be alarmed, this is normal.
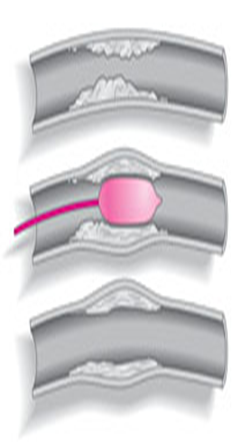
Under x-ray guidance a fine wire and tube are passed through the narrowing or blockage in the artery. A special tube with a balloon on the end of it is passed across the narrowing or blockage and the artery is then stretched by inflating the balloon. The balloon is then deflated and removed from the artery. Further pictures are taken to check if the angioplasty has been successful.
The angioplasty may need to be repeated. If the angioplasty fails to improve the blood flow, a metal scaffold (stent) can sometimes be placed in the artery. Once the stent is in place it cannot be removed and will eventually become covered by the lining of the artery.
Do I need to come into hospital for the procedure?
You will be sent an appointment for the pre-admission clinic where specialist nurses will assess you a few weeks before you have the procedure to check that you are fit enough to have it and to take some blood for routine tests. This will also give you the opportunity to ask any further questions you may have.
The procedure is usually performed as an in-patient. You will be asked to come directly to the ward on the morning of your procedure and may need to stay in overnight or discharged home the same day if no complications or you live with your family. Please take your normal blood pressure tablets on the morning of your operation.
The procedure generally takes about 30-45 minutes to perform. At the end of the procedure the tube will be removed and the doctor or nurse will press over the entry site in the groin or elbow for 10-15 minutes until the artery stops bleeding.
Once the bleeding has stopped, you will need to lie flat in bed initially for 4-6 hours before being allowed to sit up in bed. A nurse will escort you back to the ward after the procedure.
It is important for you to lie relatively still during this time to prevent the artery from bleeding again.
Are there any risks with the procedure?
There are potential complications associated with every procedure. The overall risk of the procedure is extremely low. The potential risks can be divided into the following categories:
At the puncture site
- Some bruising is common after an artery puncture.
- Very rarely significant bleeding from the artery or blockage of the artery can occur which may require a small operation.
- The risk of requiring an operation is less than 1%
Related to the contrast
- Some patients experience an allergic reaction to the X-ray contrast. In most cases this is minor but very rarely (1 in 3000) a reaction may be severe and require urgent treatment with medicines.
- The x-ray contrast can, in some patients, affect the kidney function. If you are likely to be at risk of this, special precautions will be taken to reduce the chances of this problem occurring.
- If you are a diabetic on Metformin tablets, you should not take this on the day of the procedure and for 48 hours after the procedure.
Related to the treatment
- Vessel blockage can occur after angioplasty of a narrowed artery. It can sometimes be treated with a stent.
- Vessel bursting following angioplasty occurs infrequently. This can sometimes be treated in the x-ray department by putting a stent with a covering around it (stent-graft) into the artery to seal the tear. If this is not possible, an operation may be required to repair the artery.
- Small fragments from the lining of the artery can occasionally break off and lodge in an artery below the angioplasty site (distal embolisation). This may also require an operation to 'fish out' the fragment if it is causing a problem with the blood flow. If a larger artery is blocked, there may be a risk of limb loss if left untreated. The likelihood of a complication from angioplasty or stenting requiring surgery to correct the blood flow is less than 1 in 100—1000 cases or 0.1% (BIAS data)
Other complications
If the artery in the elbow is used, the tube will pass one or more of the arteries supplying the brain. There is a very small risk (1 in 100 cases) that a blood clot may form and cause a stroke.
How successful is angioplasty and stenting?
Angioplasty and stenting is successful in treating PAD in the vast majority of patients (90-95%). In the small number of patients in whom the procedure is unsuccessful, a surgical bypass operation may be offered as an alternative.
Is there anything I can do to help?
Some patients may require blood thinning tablets or cholesterol lowering tablets after angioplasty and stenting to help maintain the benefit from the procedure. These will be prescribed and should be taken as instructed.
You can improve your general health by taking regular exercise, stopping smoking and reducing the fat in your diet. These actions will help slow down the hardening of the arteries caused by PAD and may avoid the need for further treatment in the future.
Please take any anti-hypertensive medications on the day of the procedure.
Consent to store your personal information
Vascular surgeons record information about surgical interventions, including angioplasty, on the National Vascular Registry (NVR). This is a secure database that is used to help monitor and improve vascular services throughout the country. Therefore, you (or your nearest relative) may be asked to give permission for your personal information to be stored on the NVR.
Although the database is a national system, strict data governance means personal details on the NVR can only be accessed by staff involved directly in an individual's treatment. Patient information is confidential and is not passed on to third parties other than healthcare professionals directly involved in an individual's care. You need to let your vascular surgeon know if you are unhappy for them to store your personal information on the NVR.
Contact Details
Secretaries at Frimley Park
Mr D J Gerrard, Mr Chong, Mr Chaudary 030 0613 2141
Mr K Jones, Mr Cleanthis, Miss Moore 0300 613 4291
Lt Col Sharrock, Mr Ali, Mr Dastur 0300 613 2487
North Hants Hospital Basingstoke Secretary 01256 313569
Wexham Park Hospital Secretary 0300 615 3352
Vascular Specialist Nurses
Claire Martin, Lead Vascular CNS – FPH 0300 613 6302
Tracey Craig, Vascular CNS - FPH
Andrea Croucher, Vascular CNS - FPH
Pabita Limbu, Vascular CNS - FPH
Kirstie Lane, Vascular CNS - WPH 07770 702053
Nessa Cababa, Vascular CNS - ASPH 07522 618600
Contact us
If you have any queries relating to this information, please contact the Vascular surgery service.
About this information
Service:
Vascular surgery
Reference:
Y/050
Approval date:
7 March 2024
Review date:
1 March 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.