Advice after your nerve block for surgery
On this page…
Diagram showing a Cholesteatoma
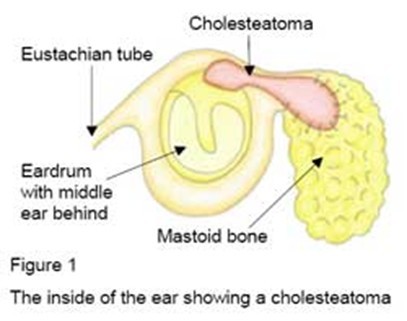
What is Cholesteatoma?
Cholesteatoma is the name for the condition in which skin becomes trapped in the middle ear and the mastoid area. As a result ear infections may occur (pain and discharge), the hearing mechanism may be damaged causing deafness and very occasionally more serious problems may arise including balance disturbance, facial weakness and infections spreading to the brain.
Several important things are in the mastoid / middle ear:
- The facial nerve—this nerve controls the muscles on the same side of the face that make all the facial expressions. The nerve lies usually in a bony canal that crosses the middle ear and mastoid.
- The hearing mechanism—the three small bones that conduct sound into the inner ear are suspended in the middle ear and mastoid.
- The inner ear and balance organ—are in dense bone adjacent to the mastoid.
Before the Operation:
You will attend a pre-assessment clinic and may have a hearing test performed. If you are taking the contraceptive pill, this should be stopped one month before surgery. If you have a cold or ear infection, your operation may be postponed.
About The Operation:
This operation is carried out under general anaesthetic (fast asleep) and can last 2-3 hours. An incision is made in the skin behind the ear. The bony surface and the honeycomb like structure of the mastoid is drilled out to clear all the cholesteatoma. This may leave a ‘mastoid cavity’ opening into the ear canal.
The eardrum also has to be peeled back to gain access to the middle ear and may be repaired at the end of the operation.
The main aim of the operation is to remove all the cholesteatoma and to stop further damage arising to the ear. It is sometimes necessary to remove some of the bones of the hearing mechanism and this may result in some further hearing loss; although reconstruction may be possible, sometimes requiring a further operation.
The ear canal opening may be enlarged to improve ventilation of the ear canal and access to the mastoid cavity afterwards.
In some circumstances a ‘second look’ into the ear may be necessary approximately one year after the first operation to ensure complete removal of the cholesteatoma.
After The Operation
A head bandage may be used and it will be removed the morning after surgery.
Any stitches that need to come out will be removed after a week.
An antiseptic dressing will be left in the ear canal for several weeks.
You will be able to go home the day after the operation but you will need to rest at home for about two weeks.
- Pain: a headache around the ear is normal and you will need pain relief for up to ten days. This will be supplied to you on leaving hospital.
- Discharge from the ear: some discharge, often blood stained, is common in the first few days but then dries up.
- Hearing: will be muffled because of the packing in the ear and tinnitus (noises in the ear) is sometimes worsened temporarily.
- Balance: is sometimes disturbed but only for a few days.
The ear may stick out a little more and will also feel numb for a few weeks. These problems will settle in time. An out-patient appointment will either be given to you when you leave the ward or be sent on later.
Post-Operative Instructions
Stay off work or school for two weeks. If the packing is to remain in the ear for longer than this you may still return to work or school with cotton wool in the ear.
Keep the ear and scar dry when washing. Cotton wool smeared in Vaseline is an effective ear plug. Avoid swimming until given the all clear.
Change the cotton wool in the ear if it becomes dirty but be careful not to pull the dressing out with it – get someone to help. If some of the dressing is pulled out cut off the bit hanging out; if a whole piece comes out contact the ward.
Minimise pressure changes in the ear - avoid vigorous nose blowing, sneeze with your mouth open. Do not fly for at least 4 weeks.
Complete any course of antibiotics you are given.
In the longer term mastoid cavities require regular cleaning of wax and should be kept dry when washing or swimming by using an ear plug.
The Risks:
The structures in the middle ear or mastoid (see above) can be damaged (very rarely) in the operation.
Tinnitus— occasionally is worsened by the operation, very rarely be damaged in the operation:
- Hearing—some hearing loss may occur from the disturbance to the bones of hearing in the middle ear. Very rarely, disturbance to the inner ear can cause complete deafness that is irreversible (only on the operated side
- Facial weakness—disturbance to the facial nerve occurs very rarely and would cause weakness of the muscles of the face on the side of the operation. It may be either temporary or permanent.
- Balance disturbance— immediately after the operation some unsteadiness may occur. Persisting dizziness is rare.
- Infection— can occur at the site of the skin cut or in the mastoid causing increased pain, discharge, swelling and fever; seek attention if you are concerned this may be developing.
- Taste disturbance— occasionally this is noticed.
- Ear discharge— occasionally a mastoid cavity or ear drum fails to heal completely. This may lead to continued discharge from the ear over the long term.
Contact:
If any of these problems arise after you have gone home please contact the wards at
Frimley Park Hospital on:
Short Stay Surgery ward Direct No: 0300 613 3216
F1 (children’s ward) 0300 613 4252
Any questions?
The team involved in your care have written this information booklet to make your admission/treatment and care as smooth as possible. However, it does not cover every aspect of your care and the staff will always be happy to answer any other questions or points of concern.
Sources of Additional Information:
British Association of Otorhinolaryngologists: www.
National Institute for Health and Clinical Excellence (NICE) : www.nice.org.uk
Contact us
If you have any queries relating to this information, please contact the Ear or nose and throat (ENT) service.
About this information
Service:
Ear, nose and throat (ENT)
Reference:
G/005
Approval date:
23 February 2026
Review date:
1 February 2029
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.