Advice after your nerve block for surgery
On this page…
Introduction
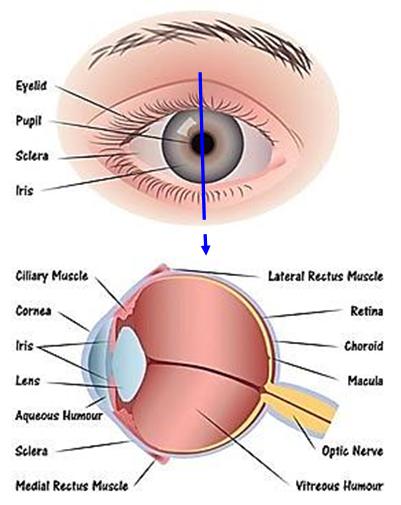
A vitrectomy is a surgical procedure that involves the removal of the vitreous gel, this is the clear jelly-like fluid located in the centre of the eye. A vitrectomy may be necessary for a number of reasons and is usually part of another operation. For example, to repair a retinal detachment, repair of macular hole, epiretinal membrane peeling, or for severe diabetic conditions. You may hear the vitrectomy called a pans plana vitrectomy (PPV) as well.
How is the vitreous gel removed?
The vitreous gel is removed through small incisions in the sclera (the white part of the eye). It is then broken up and gently removed, using highly specialised instruments and the use of a microscope. The operation can take between 30 minutes to 2 hours, depending on the reason for the operation and can be performed under a local or general anaesthetic. This will be discussed prior to surgery with the ophthalmologist. The vitreous gel does not replace itself; it will be substituted with one of the following:
- A gas bubble, which absorbs into the tissues naturally.
- Special oil, which is not absorbed and may need to be removed surgically at a later date.
- A balanced salt solution like water.
The eye produces its own clear fluid known as aqueous humour which, once the gas or air is absorbed, will gradually fill the vitreous chamber.
Retinal holes / tears and retinal detachment
The retina is the light sensitive layer of tissue that lines the inside of the eye and sends visual messages through the optic nerve to the brain.
Small holes and tears are treated with laser surgery or a freeze treatment called cryopexy. During laser surgery tiny burns are made around the hole to seal the hole. Cryopexy freezes the area around the hole and helps attach the retina.
In some cases, retinal tears or retinal breaks can lead to retinal detachment. When the retina detaches, it is lifted or pulled from its original normal position. Symptoms include sudden or gradual increase in floaters and / or light flashes in the eye. Another symptom is the appearance of a curtain over the field of vision.
Retinal detachments are treated with surgery. In some cases, a scleral buckle, a tiny synthetic band, is attached to the outside of the eye to gently push the wall of the eye against the retina. A vitrectomy may also be performed. Gas is often injected into the eye to replace the vitreous; it pushes the retina back against the wall of the eye.
A retinal detachment can occur at any stage, it is more likely to occur in people who:
- Are shortsighted (myopic).
- Have had a retinal detachment in the other eye.
- Have a family history of retinal detachment.
- Have had cataract surgery.
- Have had an eye injury.
Between 85 - 90% of those with retinal detachment can be successfully treated with one operation, although a second treatment may be needed. However, the visual outcome is not always predictable. The final visual result may not be known for several months following surgery. Even after multiple attempts at repair, treatment sometimes fails and vision may eventually be lost. Visual results are best if the retinal detachment is repaired before the macula detaches.
Macular hole
A macular hole is a small break in the macula, located at the centre of the eye’s light sensitive tissue called the retina. The macula provides the sharp, central vision we need for reading, driving and seeing fine detail. A macular hole can cause blurred and distorted central vision. There are different stages of macula hole:
- Stage I - Without treatment, about half of Stage I macular holes will progress.
- Stage II - Without treatment, about 70% of Stage II macular holes will progress.
- Stage III - The size of the hole determine how much it will affect a person’s vision. When stage III macular hole develops, most central and detailed vision can be lost. If left untreated, a macular hole can become inoperable due to its size.
What causes a macular hole?
The centre of the eye is filled with vitreous, which contains millions of fine fibres that are attached to the surface of the retina. As we age, the vitreous slowly shrinks and pulls away from the retinal surface. Natural fluids fill the area where the vitreous has contracted.
This is normal in most cases there are no adverse effects. Some patients may experience a small increase in floaters that seem to float about in their field of vision. However, if the vitreous is firmly attached to the retina when it pulls away, it can create a macular hole. Also, once the vitreous has pulled away from the surface of the retina, some of the fibres can remain on the retinal surface and contract. This increases tension on the retina and can lead to a macula hole.
Symptoms of a macular hole often begin gradually. In the early stages of a macular hole, people may notice a slight distortion or blurriness of straight ahead vision. Straight lines or objects can begin to look bent or wavy.
Although macular holes sometimes heal themselves and do not require treatment, vitrectomy surgery is often required. The vitreous is replaced with gas and disperses on its own and the body replaces it with aqueous fluid.
Epiretinal membrane peel
An epiretinal membrane is a thin sheet of fibrous tissue that can develop on the surface of the macula area of the retina and cause a disturbance in vision. An epiretinal membrane develops as a result of cellular changes that occur in the back of the eye between the vitreous gel and the macula. In many cases this membrane remains very mild and does not have any significant effect on the macula or on a person’s vision.
In other cases, however, the membrane may slowly become more prominent, eventually creating a disturbance in the retina that leads to blurring and / or distorted vision in the affected eye. An epiretinal membrane does not make an eye go completely blind. It typically affects only the central area of vision and does not cause a loss of peripheral vision.
Epiretinal membranes can be treated with vitrectomy surgery, usually under local anaesthetic. The vitreous is removed and the surgeon can then “peel” the membrane from the surface of the macular, and then vitreous is replaced with a saline solution. Most patients will have some improvement in vision after surgery, but vision is never as good as before the eye developed the membrane. Visual improvement occurs gradually over several months.
Diabetic retinopathy
Diabetic retinopathy is the most common diabetic eye disease. It is caused by changes in the blood vessels of the retina. In some people with diabetic retinopathy, blood vessels may leak fluid causing swelling of the retina. In other people, abnormal blood vessels grow on the surface of the retina. Blood vessels damaged from diabetic retinopathy can cause vision loss in 3 ways:
- Fragile, abnormal blood vessels can develop and leak blood causing blurred vision.
- There can also be blockage of blood vessels deep in the retina called “macular ischaemia” which causes irretrievable loss of vision.
- Fluid can leak into the centre of the macula, the part of the eye where sharp, straight-ahead vision occurs. The fluid makes the macular swell, blurring vision. This condition is called macular oedema.
Often there are no symptoms in the early stages of the disease, therefore it is important to have a yearly dilated eye examination or sooner if you notice any vision changes.
During the early stages of diabetic retinopathy, no treatment is needed, unless you have macular oedema. Proliferative retinopathy is treated with laser surgery. This laser treatment helps shrink the abnormal blood vessels. Two or more sessions may be required to complete the treatment.
If the bleeding is severe or recurrent, you may need a vitrectomy. During this procedure, blood is removed from the centre of the eye and laser may be applied to any leaking blood vessels. Vitrectomy is also considered when the retina is detached due to severe diabetic retinopathy. Macular oedema can be treated with laser surgery or injections in the vitreous cavity. For laser, the doctor places several laser burns in the area of retinal leakage surrounding the macula.
Possible complications of the operations
- Cataracts - This is the most common risk in vitrectomy surgery. Cataract (clouding of the lens) progression can be quite rapid, maybe within 6 months, and may need a further operation to remove the cataract. However, combined cataract surgery with vitrectomy is sometimes performed.
- Total loss of vision.
- Infection/inflammation. Occurs in about 1 in every 1000 and can be very serious.
- Retinal detachment.
- Glaucoma.
- Macular oedema / swelling.
- Haemorrhage / bleeding.
- Further surgery may be necessary.
After the operations
You should NOT fly while you have gas in your eye as the changes in air pressure can increase eye pressure. It usually takes up to 12 weeks for the gas to disperse; your surgeon will advise you.
After the vitrectomy a face-down recovery period is sometimes necessary. This is known as “posturing” and will be discussed prior to surgery. Vision improvement varies from patient to patient. Visual recovery can continue for many months.
If you have any concerns after your operation, please contact the staff in the eye treatment centre on the following numbers:
| From 9am to 5pm Monday to Friday: | |
| From 5pm to 9am and at weekends: | 0300 614 5000 and ask for the eye doctor on call |
Contact us
If you have any queries relating to this information, please contact the Ophthalmology service.
About this information
Service:
Ophthalmology
Reference:
QQ/048
Approval date:
5 August 2024
Review date:
1 July 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.