Advice after your nerve block for surgery
On this page…
What is an Anterior Cruciate Ligament (ACL)?
The ACL is one of four important ligaments which stabilize the knee joint. The ACL is found in the centre of the knee and connects the femur (thigh bone) to the tibia (shin bone). One of its most important functions is to stop the knee collapsing and giving way when you pivot (twist) upon the knee.
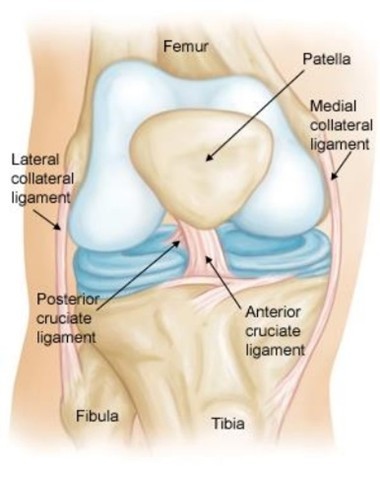
Figure 1 shows normal knee anatomy
What are the treatment options?
Rupture of the ACL is a serious injury to the knee and has become a common problem with increasing sporting activity and leisure time. The ACL is an important and strong structure which can never truly be replaced. Following even the most effective surgery the knee will never be as good as new. The ACL is not always injured in isolation – you may well have damaged bone, cartilage, and other ligaments and tendons.
Many people can manage quite well with a ruptured ACL. However, in others the knee may ‘give way’ or ‘pivot’ in an abnormal way. If these abnormal movements go on for many years, it can cause subsequent damage to other structures within the knee. The accumulated damage to the shock-absorber cartilage (meniscus) and knee joint surfaces (chondral cartilage) may increase the possibility of symptomatic arthritis in later life.
Following ACL injury, the options are to avoid situations where the knee is likely to give way; physiotherapy; or have an ACL reconstruction. ACL reconstruction must be followed by at least a nine-month programme of physiotherapy before it is safe to return to contact sport.
People for whom work or sport involves changing direction at speed (pivoting) or carrying heavy loads while turning or on uneven ground often require an ACL reconstruction.
People who run in mainly straight lines on flat ground or do no regular sport or whose work is mainly sedentary tend to find the knee has adequate stability without ACL reconstruction. Physiotherapy aims to increase the strength of core, gluteal and thigh muscles, and to improve your awareness of the position of the knee.
What are the benefits of an operation?
Most patients who wish to return to pivoting sports find they require an ACL reconstruction to provide adequate stability to the knee. In addition, a small number of patients find that, despite diligent efforts with physiotherapy, their knee is unstable during day-to-day activities. These patients may also benefit from ACL reconstruction.
An ACL reconstruction is performed to provide stability during pivoting activity. ACL reconstruction should not be expected to provide pain relief at other times. Particularly if there is already established arthritis, meniscal cartilage deficiency, or malalignment, and ACL reconstruction alone will not usually improve pain.
What would happen if I did not have an operation?
If the ligament is not reconstructed, particularly in the young active patient, then the knee may continue to give way causing further damage. The injury to the ligament together with associated damage may increase the risk of arthritis developing in later life. Surgery will not necessarily prevent joint arthritis occurring, but it is reasonable to believe that further damage to the joint will be reduced if the surgery is successful.
Are there any alternatives?
Activities that cause the knee to be unstable can be avoided. Physiotherapy can help to strengthen the knee muscles to give a degree of stability following a rupture of the ACL. Some patients, particularly those who do not do sports, are able to continue without surgery, but for those who want to return to a sport then the knee may not be stable enough.
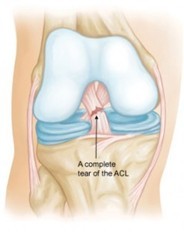
Figure 2 shows a complete ACL rupture
What does the operation involve?
- Addressing the ACL injury and any additional instability
- Addressing any associated damage inside the knee: meniscal surgery, chondral cartilage surgery
Addressing the ACL injury
Historical evidence suggests the ACL can only be successfully repaired in very select cases. Repair involves stitching the torn ACL back to the bone from which it has torn. The majority of published evidence describes reconstruction of the ACL. Reconstruction involves re-building the ACL using tissue taken from elsewhere. A number of different sources of tissue exist:
- Hamstring tendons. This is the most commonly used source in the UK. The hamstring tendons used are called gracilis and semitendinosis. They can be felt as firm cords at the back of the knee on the inner side running up the thigh. They can be taken from the thigh through a small incision at the front of the knee. Other than track sprinters (under 400m) few patients notice any loss in performance, and there is some evidence to show that they do grow back to some extent.
- Patella tendon. This is the second most commonly used source in the UK. The patella tendon runs from the bottom of the patella (kneecap) to the top of the tibia (shinbone) at the front of the knee. The central one-third of the tendon is used leaving behind two-thirds which is stitched together. This provides a strong graft, but may be associated with greater risk of long-term ache at the front of the knee, particularly in patients who spend more time kneeling, or require explosive knee extension (jumpers or kickboxers)
- Quadriceps tendon. This is used with greater frequency in recent years, but still much less frequently than hamstring or patella tendon grafts. The quadriceps tendon connects the top of the kneecap to the quadriceps muscles. The central one-third is used, and the remaining two-thirds stitched together. This provides a graft with similar strength to the patella tendon but may be associated with less long-term ache at the front of the knee.
- Donor tendon (allograft). In rare instances a frozen tendon from another person can be used. This is often because the hamstrings tendons or patellar tendon has already been used in that patient. These tissues are obtained from a national blood bank which tests all tissues for transmissible viruses (such as HIV and Hepatitis viruses) prior to use.
The surgeon will discuss with you prior to surgery which type of graft he will use and why. The new ligament is inserted into tunnels drilled into the femur and tibia using a ‘key-hole’ technique and secured with small metal or plastic screws that remain inside the bone
Extra-articular tenodesis: In knees which are most unstable, or in which ACL reconstruction has previously failed, there is some evidence that an extra-articular tenodesis may help to improve stability and prevent the new graft from tearing. This will involve an incision of approximately 10cm and reinforcement of tissue on the outside (lateral aspect) of the knee.
Addressing any associated damage inside the knee: meniscal surgery, chondral cartilate surgery
At the time of the ACL reconstruction the surgeon can identify and treat any additional damage to the knee. Most commonly this involves repair or removal of torn meniscal cartilage, or an operation to stimulate the filling of divots in the joint surface. Operations to repair cartilage often require that you wear a brace and use crutches for six weeks, and some require that you do not stand on the leg during that period. In many cases these injuries are identified on your MRI scan, but in other cases the damage is not fully visible or occurs after the MRI scan. It is important that you plan for this possibility when you accept a date for your operation.
What happens before the operation?
It is important that the knee is in good condition at the time of surgery. If the knee is swollen or stiff, the results of the reconstruction are not as good. It is important that the quadriceps muscle at the front of the thigh and hamstring muscles at the back of the thigh are as strong as possible at the time of surgery. There should be full range of movement in the joint especially straightening the knee. Activities such as swimming and cycling are preferable to running and jogging to reduce the weight-bearing load on the knee.
You will be referred to the Physiotherapy department for prehabilitation. They will be able to advise you on exercises to do whilst you are waiting for surgery and how to ensure your knee is optimally prepared for the surgery.
As your knee is unstable it is advisable to avoid the following movements:
- Turning sharply on your knee
- Twisting
- Jumping
- Sharp acceleration and deceleration
- Change of direction at speed and walking
- Jogging or running on uneven surfaces.
If you cannot get your knee fully straight before the surgery, and the MRI scan shows that torn cartilage may be blocking the movement of the knee, it may be necessary to repair/remove the torn cartilage during a preliminary operation, then return approximately 6 week later to reconstruct the ACL once the knee can straighten fully.
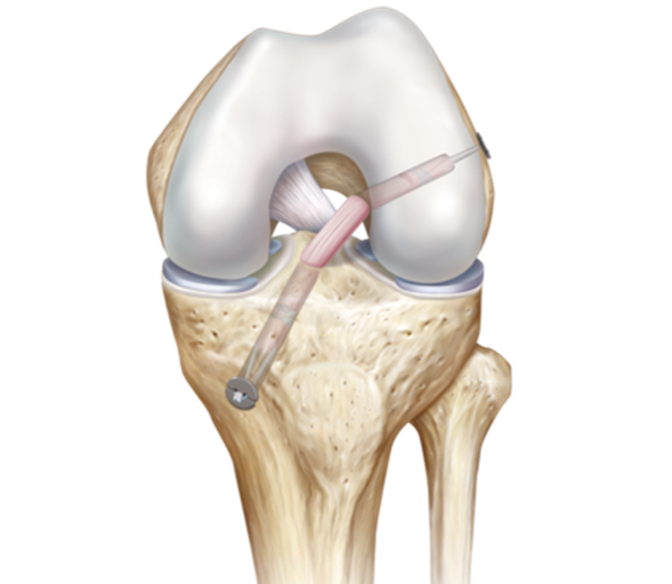
Figure 3 shows the knee following ACLR
The National Ligament Registry (NLR)
In order for us to keep an accurate record of the type of surgery on your knee, the medical devices used to fix the new ligament, and your outcome following surgery, we may ask that you register with the National Ligament Registry.
On the day of your operation
You will be admitted to the day surgery unit on the morning of your operation. You will be admitted to the unit and see by the surgical team, an anaesthetist and the therapy team prior to your surgery, You will have the opportunity to ask questions/address any concerns.
What happens after the operation?
Following your operation, you will wake up in the recovery area of the theatre. Your knee will be in a bandage and you will have an ice pack on your knee. Ice can be beneficial in the management of post-operative swelling and pain. The dressing on your knee will be taken off before you go home. The wounds will be covered by small dressings and these should not be removed (but can be changed if needed). At rest the knee should be kept as straight as possible.
On your return to the day surgery unit you will see the Physiotherapist, who will teach you some specific exercises, teach you how to mobilise safely with crutches and complete a stair assessment. The Physiotherapist will confirm how much weight you can put through your leg after the operation. If you have had a meniscal repair or cartilage surgery, you may be in a brace and the amount of weight you can put through the leg may be altered. The Physiotherapists on the ward will explain this to you when they assess you after the operation.
Depending on the timing of your operation and the complexity of your individual case you can expect to be discharged from hospital the same day of your operation. You will need to continue your exercise programme at home as instructed by the Physiotherapist on the ward.
Patients with a personal or family history of clots in the leg or lungs may be asked to take some medication to prevent clot formation. Usually this is just a single dose on the day after the operation, but the prescription may be extended if the patient will not be putting any weight on the leg.
You will be seen by an outpatient Physiotherapist shortly after your operation. You will be given the appointment before you are discharged from the ward. At this appointment they will check your wound and assess your knee and mobility. If it is appropriate, they will introduce some new exercises to continue at home.
Your rehabilitation will begin from two weeks post-surgery. ‘Standard’ ACL rehabilitation can be divided into three phases:
Phase 1 Early recovery
Phase 2 Initial strengthening (2 weeks – 6 weeks)
Phase 3 Functional recovery (6 weeks – 6 months)
Phase 1 (Early recovery)
Aims of treatment at this early stage are:
To reduce swelling of the knee
To regain muscle control
To regain movement
To restore a normal walking pattern
The early post-operative period is a very important phase in the recovery process. As individuals vary, progress can be variable but there are some important principles that need to be considered.
Reducing swelling
The knee must be allowed to recover from the operation. Inevitably there will be pain, stiffness and swelling for the first 2 weeks. Therefore, the knee needs to be rested adequately. This means that you should spend time sitting/lying with the leg elevated. Swelling of the knee and leg is very common. You may also find that there is bruising to the shin and at the hamstring donor site. The best way to minimize any swelling is to elevate the leg so that the foot is higher than the hip. This can be done by elevating the end of your bed or putting pillows under your ankle and heel, the knee should also be supported. If sitting in a chair it is best to elevate your leg on a chair or a stool with the knee supported. Ice packs will also help to reduce swelling and bruising.
Regaining muscle control and movement
Regaining full extension (straightening) of the knee is vital to the success of the operation. You will therefore be encouraged to straighten your knee fully from an early stage. It is quite safe to move your knee immediately after surgery and you will be encouraged to do so. As stated previously, regaining full extension (straightening) is of prime importance but it is also important to flex (bend) the knee. Most people will be able to achieve 90 degrees of flexion (a right angle) after a few days. You should not rest with a pillow or cushion under the operated leg.
Restoring a normal walking pattern
Following your operation, it is quite safe to take full weight through your operated leg, however elbow crutches are used as it may be uncomfortable at first. If you have had meniscal or cartilage surgery, this may be different. You will be aware of this before you are discharged home from hospital.
At home and up to two weeks after surgery
The knee should be rested and elevated when you are sitting down, with the knee supported. Then movement of the knee should gradually be increased. You should have full extension and at least 90 degrees of flexion by 2 weeks. Painful bruising, swelling, redness and inflammation down the front of the shin and ankle can occur after 4-5 days due to the joint fluid (synovial fluid) leaking out of the front of the knee and tracking downwards due to gravity. This tends to settle down by 7-10 days when the joint is fully sealed following surgery. The discomfort can be minimized by elevation, which will reduce the gravitational effect. You will be encouraged to increase mobility, including weight bearing as pain permits.
Phase 2 (Two weeks – six weeks)
At your 2-week appointment a nurse will check your wounds and if there are stitches to remove this will be done then.
Outpatient physiotherapy begins at this stage. It is very important that you attend your physiotherapy sessions and comply with their advice for you to achieve the optimum outcome from your surgery.
The aims at this stage are:
- Fully extend and flex (bend) the knee
- Strengthen the muscles around the knee joint
- Improve balance and to teach correct walking
The exercises given to you by the physiotherapist are ‘closed chain’ rather than ‘open chain’. This means that the foot of the operated leg is in contact with another surface (as on the pedal of a bike), therefore closing the chain of joints in the leg. The reason for this is that it reduces stress on the new ligament, which is vulnerable in the early weeks following surgery.
The Physiotherapists will advise you about the exercises you should do, and you may be referred to a group exercise class. You will also be given advice about exercise you can do in your local gym and at home.
At the end of the first 6 weeks the knee should have full range of movement.
It is normal in the 2-6 week phase to feel tightness and pulling in the hamstrings if you have had a hamstring tendon reconstruction. Recent scientific evidence has shown the hamstring tendons re-grow after they have been removed and this sensation is the new tendons re- growing; they may feel tight around the knee area.
Phase 3 (Six weeks – six months)
You will continue with your rehabilitation programme, guided by the Physiotherapists. This concentrates on the return of muscle function, balance work (proprioception) and range of movement. There is a gradual increase in the level of activity with ‘straight line’ work, initially avoiding movements that put the knee at risk, for example turning, twisting, jumping; sharp acceleration and deceleration, change of direction at speed; and walking, jogging or running on uneven or unpredictable surfaces.
After 12 weeks the physiotherapists will advise you about gradually introducing these activities. The Physiotherapists will also advise you and help you with sport specific rehabilitation for your particular sport or activity. You need to be prepared to commit to doing a gym based programme 4 times per week to achieve the full benefit of your surgery.
Your physiotherapist will continue to instruct you on suitable exercises for you and it is important that you only do the exercises that they give you, in order to protect the graft. It is important that you do these exercises at home or in your local gym, you may not be coming to physiotherapy to do these sessions.
What activities will I be able to do afterwards?
At 6 months there should be full range of movement in the knee. At this stage it should be safe to return to non-contact sports e.g. distance running, gym based classes and programmes. From 6 months you should continue to exercise to return to all normal sporting activities. In most cases contact sports can be resumed from around 9 months and winter sports from 1 year. Please remember every patient is different and the speed of your return to sport is variable and will depend on a number of factors including the severity of the injury to your knee. Your surgeon will advise you when your return to sport is likely to be. For younger patients, your surgeon may advise that you do not return to contact sport until 1 year following surgery.
When can I return to work?
You may return to sedentary work (non-physical) at approximately 2-3 weeks. However, return to light physical work should be delayed for at least 6 weeks and heavy physical work for 3 months following surgery. You should discuss your return to work with your Doctor; it is advisable to start with light duties first.
When will I be able to drive?
Driving should be possible at 6 weeks. If you drive an automatic car and have had your left knee operated on, you can drive after 2 weeks.
What about wound care?
You will be seen by the nurses 1-2 weeks following your surgery. Any sutures will be removed or trimmed at this time. If the wound is fully healed, no further dressings will be required. Once your dressings have been removed it is safe to get the wound wet.
Depending on the complexity of your operation, some procedures have longer recovery times. This should have been discussed with you during your appointment with your Consultant. Your post-operative recovery will be discussed with you before you leave the hospital
What are the risks?
There is no surgical procedure that is free from complications. ACL reconstruction has a very good record of safety and success, but complications can occur.
COMMON (2-5%)
- Pain: the knee will be painful after the procedure. Pain killers (Analgesics) will be given to prevent this including enough to go home with.
- Numbness: the skin around the knee or shin may be temporarily or more permanently numb due to damage of small nerves.
- Swelling/ Hemarthrosis: This is a collection of fluid or less commonly, blood in the knee joint. In most cases, the body will absorb the fluid itself. If the swelling becomes too large, the surgeon may feel an operation is necessary.
- Stiffness: you may have difficulty in straightening your knee or squatting.
- Persistent pain: pain may persist after the procedure. A repeat arthroscopy or further surgery may be required.
- Continued instability: weakness and instability may occur despite adequate surgery
LESS COMMON (1-2%)
- Infection: the wound sites may become red, painful and hot. There may also be a discharge. These are signs of infection and can usually be treated by antibiotics. The infection may spread to the knee joint itself (requiring a washout) and removal of the graft. Infection may also spread to the blood (sepsis) requiring intravenous antibiotics.
- Graft rupture: (torn graft) this may occur after further trauma. Further surgery may be necessary.
- DVT/ PE: These are blood clots in the calf/ leg and if they travel to the lungs may be fatal
RARE (<1%)
- Damage to structures within the knee: this is rare but may cause further damage and symptoms. This may need further treatment including operation. These include fractured kneecap (patella) if a patellar tendon graft is used.
- Damage to the skin under the tourniquet: this may require dressing, surgery or skin graft. There may also be numbness of the skin under the tourniquet, this is usually temporary.
- Damaged instruments: these may break within the knee and require an opening of the joint to remove them.
- Abnormal wound healing: the scar may become thick, red and painful (keloid scar).
- There may also be delayed wound healing for numerous reasons.
- Compartment syndrome: this is a build-up pressure within the lower leg and can cause nerve damage, blood vessel damage and muscle damage. If this occurs, an emergency operation is required to prevent death of tissue.
- Osteoarthritis: this can be more common after joint operations.
- The risk of graft rupture is dependent on a number of factors and unique to an individual patient. Overall, the risk of graft rupture is approximately 5% by two years after the surgery (1 in 20 patients). However, this figure may be higher in younger patients, and those returning to high demand sports.
Useful Contacts
Heatherwood Hospital:
- Orthopaedic pre assessment 0300 614 7778 / 0300 614 7147
- Arthroplasty Nurse Heatherwood 07789927177
- Nurses Station Treetops Heatherwood 0300 614 4175
- Physio/OT Office Treetops Heatherwood 0300 614 4178
Frimley Park Hospital:
- Frimley Park Physiotherapy 07570 974390
- S2 Elective Ward Frimley 0300 613 3781 / 0300 613 3783
- Elective Helpline Frimley 0300 613 2556
Wexham Park Hospital:
- Ward 1 Wexham Park 0300 615 3010 / 0300615 3012
- Outpatient Physio Wexham 0300 615 3501 / 0300615 3500
- Wexham Park Physiotherapy 07717 199851
Contact us
If you have any queries relating to this information, please contact the Orthopaedics service.
About this information
Service:
Orthopaedics
Reference:
N/009
Approval date:
24 June 2025
Review date:
24 June 2028
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.