Advice after your nerve block for surgery
On this page…
Why do I need an Adenosine test?
Your doctor has advised you to undergo an Adenosine test as he/she suspects you have an accessory (extra) pathway.
The normal electrical system of the heart
The heart is, in the simplest terms, a pump made up of muscle tissue. The heart's pumping action is regulated by an electrical conduction system that coordinates the contraction of the heart chambers.
The conduction system sends signals throughout the upper (atrial) and lower (ventricle) chambers of the heart to make it beat in a regular, coordinated rhythm. The conduction system consists of two nodes that contain conduction cells and special pathways that transmit the impulse. The normal heartbeat begins when an electrical impulse is fired from the sino-atrial (SA) node in the right atrium. The SA node is responsible for setting the rate and rhythm of the heart and is therefore referred to as the heart’s ‘pacemaker.’
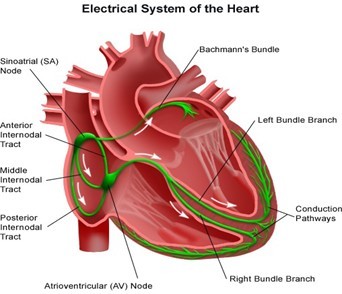
Normally at rest, as the electrical impulse moves through the heart, the heart contracts about 60 to 100 times a minute depending on a person's age. This is referred to as a normal sinus rhythm.
What is an Arrhythmia?
Sometimes if the conduction pathway is damaged, becomes blocked or if an extra pathway exists, the heart rhythm changes. The heart may beat too quickly (tachycardia), too slowly (bradycardia), or irregularly, which may affect the heart’s ability to pump blood around the body.
These abnormal heart beats are known as arrhythmia. Arrhythmias can occur in the upper chambers of the heart (the atria), the lower chambers of the heart (the ventricles), and at the junction between the atria and ventricles.
Supraventricular Tachycardias
Supraventricular tachycardia (SVT) is a tachycardia arising from above the ventricles causing the heart rate to exceed that of normal. SVTs may include AV nodal re-entry tachycardia (AVNRT), AV re-entry tachycardia (AVRT), Atrial tachycardia.
Atrial fibrillation and Atrial flutter are also classified as types of SVT.
The most common type of SVT is AVNRT. In AVNRT an electrical pathway exists that bypasses the normal conduction system. The pathway directly connects the atria to the ventricles. This extra pathway is known as an accessory pathway. The electrical impulses travel along the accessory pathway, therefore bypassing the AV node, which normally acts as a gateway to the ventricles.
The tissue in the extra pathway does not slow the electrical impulses down, as happens in the AV node, therefore the electrical impulses reach the ventricles ahead of the ‘normal’ electrical impulses (this is known as pre-excitation). Most patients with AVNRT don’t have structural heart disease, and it is most often seen in young healthy women. However, some patients do have underlying heart disease such as pericarditis, or a previous heart attack.
The second most common type of SVT is AVRT which is typically present at a younger age than those with AVNRT. The third most common type of SVT is atrial tachycardia.
What is Adenosine?
Adenosine is a naturally occurring substance found in all of us, in small quantities, in all cells. It is routinely used to diagnose and treat abnormal heart rhythms. Adenosine slows down the electrical impulses between the upper (atrial) and lower (ventricles) chambers of the heart.
This slows the fast or uneven heart beats called ‘arrhythmias,’ and helps the doctor to find out what type of arrhythmia you have so that a management plan can be put in place.
What preparation is needed for an Adenosine test?
Avoid caffeine on the day of the test. On arrival at the ward, you will be introduced to the nurse who will be looking after you. The nurse will explain the procedure to you and answer any worries or questions. Before the procedure, the nurse will take your blood pressure and heart rate and then use a small needle to insert a plastic tube (cannula) into a vein in your arm; this will allow the nurse to give you Adenosine. The nurse will take blood and record an ECG. The nurse will explain the risks of the procedure and obtain your verbal consent.
What are the possible side effects/complications?
Complications associated with this procedure are very rare. Like all medication, Adenosine can cause side effects, although not everybody gets them.
It is common to experience a metallic taste in your mouth during administration of Adenosine. You may be aware of skipped heart beats or extra heart beats, and your heart racing. Also, as Adenosine will cause your heart to go into a slow rhythm, you may feel dizzy or experience visual disturbances, such as double vision. Because the Adenosine will cause your heart to go into a slow rhythm, if your heart does not recover quickly, you may need external pacing to regulate your heart rhythm.
You may also have some chest pain or pressure on your chest, shortness of breath or an urge to breathe deeply, and a flushed hot feeling.
The side effects normally settle within seconds or minutes after the injection is finished.
What happens during the Adenosine test?
During the procedure you will be awake and able to talk. For the duration of the test, you will be connected to the ECG machine.
The nurse will administer the Adenosine rapidly via the cannula in your arm whilst the ECG is continuously running. If you experience any uncomfortable symptoms during the test, please inform the nurse.
After the Adenosine Test
You will then be offered a drink and have your blood pressure and pulse checked again. The nurse will show your ECGs to the Consultant who will discuss the findings with you. You will be kept in a monitored bed for approximately 30 minutes to 1 hour before you are discharged home.
You are allowed to drive yourself to and from the hospital. You can resume normal daily activities and return to work upon discharge.
More information can be found at the following websites:
SADS UK at www.
Tel: 01277 811215 Email: info
Cardiac Risk in the Young (CRY) at www.
Tel: 01737 363222 Email: cry
British Heart Foundation at www.
Tel: 0300 330 3322 Email: supporterservices
Arrhythmia Alliance at www.
Tel: 01789 450 787 Email: info
Contact us
If you have any queries relating to this information, please contact the Cardiology service.
About this information
Service:
Cardiology
Reference:
C/015
Approval date:
7 August 2025
Review date:
1 August 2028
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.