Advice after your nerve block for surgery
On this page…
Introduction
You have been offered surgery for your frozen shoulder. The aim of this leaflet is to give you a general understanding of your condition and what to expect both before and after your operation. It is designed to help you to prepare for your operation and its recovery.
What is Frozen shoulder (also called Adhesive Capulitis)?
The lining of the shoulder joint is known as the ‘capsule’ - this thin structure keeps the lubricating joint fluid within your shoulder. It’s normally thin and flexible and this allows the shoulder to have great mobility. In frozen shoulder, this capsule becomes inflamed, thickened and tight and this results in pain and stiffness
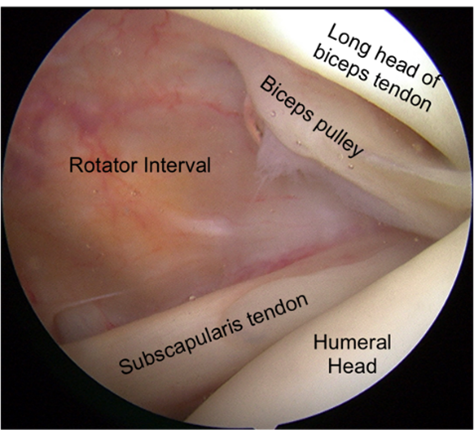
Figure 1 normal shoulder inside view – note the appearance of the rotator interval
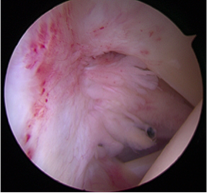
Figure 2 frozen shoulder inside view - thick, red inflamed tissue filling and shrinking the rotator interval
The condition usually goes through three phases, starting with pain that can be very intense and it often comes on out of the blue. Stiffness then develops and for many the intensity of the pain gradually reduces. Finally a thawing stage occurs where the pain eases and most if not all movement returns. This process may take a long time, sometimes as long as three years.
The severity of frozen shoulder symptoms can vary widely: some patients experience only mild discomfort and stiffness, while others suffer debilitating pain and stiffness that makes daily living very difficult.
Why have I got a frozen shoulder?
Frozen shoulder is a common condition. Most patients are middle aged and women suffer more often than men. People with diabetes or thyroid disease are more at risk.
For many patients there is no identifiable cause, but frozen shoulder sometimes follows an injury or surgery to the shoulder. This is called a 'secondary frozen shoulder'.
Before you are offered surgery for your frozen shoulder, you may have already tried a special injection (US-guided hydrodistension) and physical therapy. This helps two-thirds of patients get enough relief that they do not need an operation. If your frozen shoulder has not not settled enough then surgery may be required to help you with your problem.
Surgery for frozen shoulder: What is Arthroscopic Capsular Release and Manipulation Under Anaesthetic (MUA)?
This is a keyhole operation on your frozen shoulder. It is usually done as a day-case procedure under a general anaesthetic with a regional nerve block (an injection that numbs the shoulder and arm).
Tiny incisions are made to allow telescopic instruments to enter your shoulder joint. The inflamed capsule is released from the inside. The shoulder is then carefully manipulated by your surgeon to achieve complete release of the capsule. This should allow significantly improved range of motion in your shoulder.
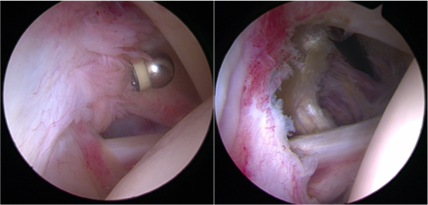
Figure 3 keyhole instrument is being used to remove the inflamed capsule before manipulation
You will wake up with your arm in a sling and there will be dressings on your shoulder.
What are the benefits of this surgery?
This operation has a high chance (85-90%) of significantly improving both your pain and your stiffness. The improvements may occur very quickly (within 2-4 weeks) but some patients will take longer to recover (up to 4 months).
These improvements in pain and motion significantly improve patients’ ability to sleep and to function for normal daily activities as well as for work, hobbies and sports.
How much pain will I be in after the operation?
When you first wake up from your surgery, you will probably be comfortable as the regional nerve block will be making your whole shoulder (and arm) numb.
You will go home on the same day as your operation. We will give you medications to take home that help with post-operative pain.
As your regional block wears off (normally between 8-24hrs post-op) you will start to feel pain in your shoulder. At this time you should start taking your painkillers and continue to take them regularly for the first four days after your operation. After this, you can wean down to simple paracetamol and ibuprofen (if tolerated) as your pain allows and then to nothing. Most patients will be off all painkillers by three weeks after surgery, but some patients experience pain for longer. Making sure your pain is well controlled will also enable you to do your exercises more easily in the first few days after your operation. If you are struggling with pain post operatively and it is impeding your ability to move your arm please get in touch with the nurse care team on 0300 614 4130/ 0300 614 4131
What is my post-operative rehabilitation?
You will be seen by a physiotherapist on the day of your operation and they will teach you how to do the correct exercises after surgery and give you this information sheet take home.
To get the best movement recovery from your operation, it is very important that you engage with your post-operative physiotherapy program. This means you need to do your exercises 5-6 times a day at home and attend regular out patient physiotherapy appointments. If you do not do these exercises, it is probable that your final result will not be as good.
What are the Alternatives to Surgery?
Physiotherapy
Physiotherapy doesn’t usually work too well on its own in the early stages of frozen shoulder. However Physiotherapy is essential following surgery, and it is vital you do your exercises regularly to achieve and maintain the range achieved in surgery.
Steroid Injection (Cortisone)
It is likely you have already tried some form of injection therapy (steroid injection and/or hydrodistension) before you were offered surgery for your frozen shoulder. If you have not yet had an injection, you may wish to try this before surgery.
What happens before your admission to hospital?
You will be contacted by the bookings team to arrange your surgery date. You will need to attend the pre-operative assessment clinic to assess your fitness for surgery.
At the time of listing for surgery, you will have been given information regarding your surgery, and an opportunity to ask questions. This information leaflet should also help you to understand the pathway.
Coming into hospital
You will be told when to arrive at the hospital on the day of your surgery. Please do come on time so we can get you ready in time for your operation.
Please do not eat any food for 6 hours prior to your surgery. You can drink water until your surgery. You may be given a small carbohydrate drink 2 hours prior to your surgery when you are with us.
You will normally go home on the same day as your surgery. There are many advantages to being in your own environment, reducing the risk of complications and being in control of your own recovery. In some rare cases, your consultant may ask you to stay overnight and go home the following morning. If this if required, you will be made aware of this prior to your admission.
You will need to arrange for someone (e.g. a family member or a friend) to bring you to and from the hospital as you will not be able to drive home after your operation.
What do I need to do after my surgery?
Pain relief
It is important to take your painkillers as prescribed to keep pain to a minimum. This will also enable you to do your exercises more easily in the first few days after your operation. Ice can be helpful to reduce pain/swelling. Protect your dressings from getting wet with a plastic bag. Wrap a bag of ice/frozen peas in a damp towel and apply for 10-15 minutes. This can be repeated every 3-4 hours.
Wound care
Following your operation, you will usually have 2 tiny (<1cm) wounds, one at the front and one at the back of the shoulder and these will be covered with a dressing. Your wounds need to be kept clean and dry until they have healed (usually about 10 days). The nursing staff will provide you with more information about wound care on discharge. At 2 weeks after your operation you will attend a nurse physio/led clinic for your wound to be checked.
Sleeping positions
Sleep is important in your recovery, and can be a bit of a challenge after an operation. Here are some tips that may help:
- Take your painkillers just before bed.
- You may find the following sleeping positions helpful. Use pillows to help support your operated arm as shown below.


Rehabilitation
With frozen shoulder surgery it is very important that you begin to move the arm as soon as possible to maintain the amount of movement that the surgeons have achieved.
Your sling is for comfort and safety while your nerve block is still active. You should remove it the day after your operation once you have regained sensation and control in your arm and begin your exercises. The more times that you can do your exercises after your operation the better. You should aim to complete the exercises a minimum of five times a day. If you need to rest the shoulder in your sling between sessions for an hour or so over the first few days that is fine, but try to wean off the sling altogether by day 5 post-op.
You will have been seen by the therapist on the day of your surgery. They will go through the exercises with you. You will be given an appointment for outpatient physiotherapy within a few days of your operation. For the first couple of weeks after the operation you will likely have 2 sessions a week (it is very important that you attend these appointments in addition to doing your exercises 5-6 times a day at home – they are key to the success of this procedure). Your therapist will check how you are progressing with your exercises but will also help you to regain your motion.
Repeat all exercises below 10 times each.
Capsular release exercises - Standing table slides
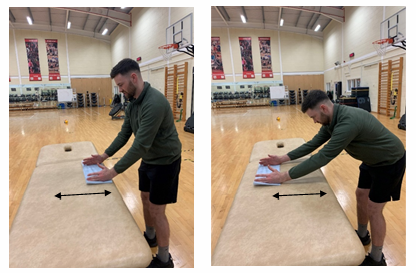
- Stand in front of a table or a countertop.
- Place both hands on the table onto something that slides easily, like a towel or cloth. Bend forwards from your hips and slide your hands forwards on the table.
- Keep your elbows straight and your neck and shoulders relaxed.
- Hold for a moment and return to the starting position.
- Repeat 10 times
External rotation with stick

- In standing, maintain a good posture, place a folded or rolled up towel between the affected arm and your side.
- Hold a stick with both hands, shoulder width apart.
- Keeping your elbows in, use your unaffected arm to push the bar outwards helping your affected arm rotate.
- Take you arm to the beginning of the stretch.
External rotation at 90 degrees abduction
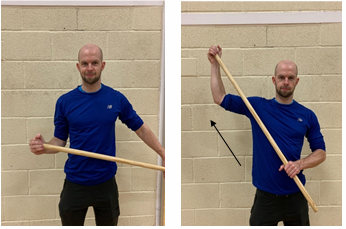
- In standing, holding a stick in both hands. Take your affected arm out to the side and up to 90 degrees.
- Use the stick to apply gentle pressure at the end of the movement (within comfort).
- Hold for a few seconds and then return to the starting position.
Hands behind back

- Holding onto an empty Kitchen roll tube with affected side, place hand behind your back.
- Pass the tube to your opposing hand and bring the tube in front of you.
- Place the tube back into your affected side and repeat this movement. If this becomes too easy, use a smaller tube to ensure you have to move your arm further.
When can I return to work?
If you have a desk job you can return to work after a week, If your job involves lifting or manual work you may need longer.
When can I drive?
You can normally return to driving at 1-2 weeks
When can I return to sporting activities?
Your physiotherapist will give you guidance on this throughout your rehabilitation as your mobility and strength improves.
What are the risks and possible complications?
Keyhole surgery is generally very safe. Nevertheless, all operations carry some risks:
Anaesthetic risks: Modern surgical practice is very safe, but there are small risks associated with anaesthetics and regional nerve blocks. These risks are increased for those patients with significant pre-existing medical problems. Your anaesthetist will discuss these risks with you.
Deep Infection is very rare after keyhole surgery (<1% risk).
Major bleeding: the risk is very low after keyhole surgery (less than 1%).
Nerve injury is rare after this operation (1%). A nerve that supplies some shoulder muscles can rarely get stretched during the manipulation phase of the procedure. This may cause weakness around the shoulder but it should recover within a few months of surgery.
Shoulder instability is very rare after this operation (<1%). If it is an ongoing problem it may require further surgical treatment.
Fracture or structural injury in the shoulder is rare and will be dealt with during or after the operation if it occurs.
Post-op blood clots (DVT) are extremely rare after this procedure (less than 1%). You do not normally require any preventative medications for this after frozen shoulder surgery.
Useful Contacts
Heatherwood Hospital:
- Orthopaedic pre assessment 0300 614 7778 / 0300 614 7147
- Arthroplasty Nurse Heatherwood 07789927177
- Nurses Station Treetops Heatherwood 0300 614 4175
- Physio/OT Office Treetops Heatherwood 0300 614 4178
Frimley Park Hospital:
- Frimley Park Physiotherapy 07570 974390
- S2 Elective Ward Frimley 0300 613 3781 / 0300 613 3783
- Elective Helpline Frimley 0300 613 2556
Wexham Park Hospital:
- Ward 1 Wexham Park 0300 615 3010 / 0300615 3012
- Outpatient Physio Wexham 0300 615 3501 / 0300615 3500
- Wexham Park Physiotherapy 07717 199851
Contact us
If you have any queries relating to this information, please contact the Orthopaedics service.
About this information
Service:
Orthopaedics
Reference:
N/067
Approval date:
13 May 2025
Review date:
13 May 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.