Advice after your nerve block for surgery
On this page…
Introduction
The aim of this leaflet is to give you a general understanding of your shoulder pain and what happens before and after your sub acromial decompression +/-ACJ excision. It is designed to help you to prepare for your operation and after care once you go home.
Sub-acromial shoulder pain
Subacromial shoulder pain is the most common type of shoulder pain. It is also known as ‘rotator cuff tendinopathy’, ‘shoulder impingement’ or ‘subacromial bursitis’. It is caused by chronic inflammation in the region of the rotator cuff. It is very common, but often responds to exercise and posture correction.
What are the symptoms?
Subacromial shoulder pain is often felt around the shoulder and upper arm, but it may also be felt towards the neck and shoulder blade. It often feels worse when the arm is raised to shoulder height or reaching behind your back. Simple activities, such as reaching for items on shelves, driving or getting dressed may be painful. Sleep can also be affected, and it is often difficult to lie on that side.
Pain may come on gradually over time or can occur suddenly particularly if the shoulder has been used for an activity that is much more demanding than it is used to doing each day.
Who gets sub-acromial pain and what causes it?
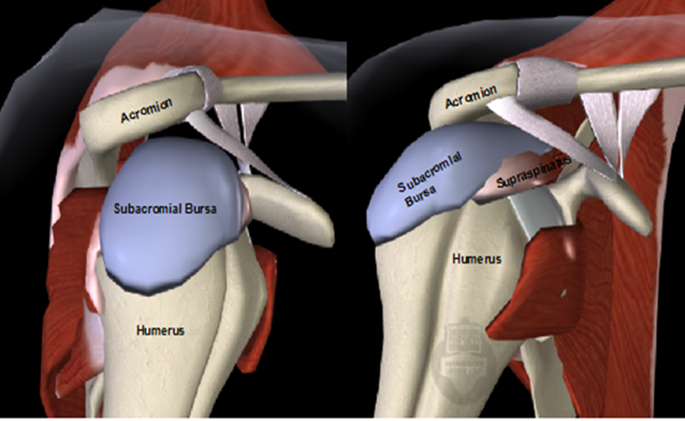
Figure 1: Graphic of right shoulder from front and side, note the blue area is the sub acromial bursa which is normal a cushion between the rotator cuff tendons and the roof of the shoulder.
Subacromial shoulder pain is very common. Most patients are between 40 and 65yrs old and it is slightly more common in women. It can develop due to age related changes, repetitive strain, increase in load, injury or even for no apparent reason. Other health factors can influence your shoulder tendon health such as: smoking, obesity, high fat diet, high cholesterol levels, low vitamin D levels, low Oestrogen (menopause) and Diabetes.
As we get older, our tendons tend to get a little weaker and it is common also to develop small bony spurs that can promote rubbing in the shoulder. Tendon degeneration and bone spurs can cause inflammation in the subacromial bursa which patients then feel as pain.
Alternatives to Surgery?
Physiotherapy
Before having this type of surgery, you should have undertaken a course of physiotherapy. There is good evidence that physiotherapy focussing on optimising posture, movement and strength in the shoulder will improve many patients’ symptoms and allow them to avoid surgery. It is important to understand it can take at least 6 weeks of strengthening and postural work before you notice improvements in your pain and function. It is therefore important that you follow your physiotherapist’s advice and exercise programme to achieve the best outcome.
Try to incorporate the exercises into your daily routine. If initially the exercises are causing some discomfort, complete them on alternate days. Significant gains can be made in strength if you do the exercises about 4-5 times a week.
Further information on exercises can be found on the BESS website. Subacromial Shoulder Pain – British Elbow & Shoulder Society (bess.ac.uk).
Steroid Injection (Cortisone)
You may have been recommended or had a steroid injection. The risks of injection are extremely low, and most patients enjoy significant pain relief, it can also be used to provide an excellent window of opportunity for you to strengthen the rotator cuff and scapula muscles with the physiotherapist, which will then help manage your problem in the longer term.
Information about the procedure
What is a Subacromial Decompression?
This is a keyhole operation that is performed under general anaesthetic and regional nerve block, it aims to remove the inflamed and thickened bursa and smooth out the bone increasing the gliding space for the rotator cuff tendons under the acromion. This makes the subacromial space larger and so reducing the pressure and friction on the tendons of the rotator cuff.
This procedure is only offered if conservative management (such as a physiotherapy strengthening programme and injections) have not helped and may be carried out in conjunction with other shoulder procedures such as an acromioclavicular joint excision (detailed below), rotator cuff repair and/or biceps tendon surgery.
An Acromial-clavicular joint excision involves removal of the under surface of both the inner part of the acromion and the end of the collar bone, the top of the joint is untouched to retain stability. This is done if wear and tear of this joint is causing your symptoms and reducing the space for the rotator cuff tendons. It is very common to get wear and tear in the acromial clavicular joint, most of us have some degree of wear and tear without it producing any symptoms or problems at all.
What happens before your admission to hospital?
You will be contacted by the bookings team to arrange your surgery date. You will need to attend the pre-operative assessment clinic to assess your fitness for surgery.
At the time of listing for surgery, you will have been given information regarding your surgery, and an opportunity to ask questions. This information leaflet should also help you to understand the pathway.
Coming into hospital
You will be admitted to hospital on the day of your surgery. Please do not eat any food for 6 hours prior to your surgery; you can have a cup of tea or coffee with a small amount of semi-skimmed milk up to 2 hours prior to surgery and you can drink water until your surgery You may also receive a carbohydrate drink 2 hours prior to your surgery.
Time spent in hospital following surgery has reduced significantly over the last few years. Changes in surgery technique and support allows patient to go home on the same day of their surgery. There are many advantages to being in your own environment, reducing the risk of complications and being in control of your own recovery.
You will need to arrange for someone (e.g. a family member or a friend) to bring you to and from the hospital as you will not be able to drive home after your operation.
What do I need to do after my surgery?
Wound care
Following your operation, you will have small (1cm) wounds, around your shoulder, where the instruments have been inserted. These will be covered with a dressing.
Your wounds will need to be kept clean and dry until they have healed (usually about 12 days). The nursing staff will provide you with more information about wound care on discharge. At 2 weeks after your operation, you will attend a nurse and physio-led clinic for your wound to be checked and the dressing is usually removed at this point.
How much pain will I be in after the operation?
When you first wake up from your surgery, you will probably be comfortable as the regional nerve block will be making your whole shoulder (and arm) numb.
You will go home on the same day as your operation. We will give you medications to take home that help with post-operative pain.
As your regional block wears off (normally between 8-24hrs post-op) you will start to feel pain in your shoulder. At this time, you should start taking your painkillers and continue to take them regularly for the first four days after your operation. After this, you can wean down to simple paracetamol and ibuprofen (if tolerated) as your pain allows and then to nothing. Most patients will be off all painkillers by three weeks after surgery, but some patients experience pain for longer.
Making sure your pain is well controlled will also enable you to do your exercises more easily in the first few days after your operation. If you are struggling with pain post operatively, please get in touch with the nurse care team on 0300 614 4130 or 0300 614 4131
Ice
Ice can be helpful to reduce pain. Protect your dressings from getting wet with a plastic bag. Wrap a bag of ice/frozen peas in a damp towel and apply for 10-15 minutes. This can be repeated every 3-4 hours.
What is my post-operative rehabilitation?
You will be seen by a physiotherapist on the day of your operation, and they will teach you how to do the correct exercises after surgery. There are no restrictions to moving your shoulder following this operation (unless you’ve also had a rotator cuff repair). It is therefore important to move your shoulder regularly, as comfort allows.
You will be seen by a physiotherapist about 2 weeks following the operation at the post-op clinic. If further physiotherapy is required it will be arranged following this appointment. Your physiotherapist will help guide your rehabilitation which will be dependent on the pain you are experiencing at the shoulder.
It can take approximately 3 months for a 50% improvement in pain, and up to 6 months to achieve an 80% improvement in function. Full recovery may take up to a year.
Sleeping positions
Sleep is important in your recovery and can be a bit of a challenge after an operation. Here are some tips that may help:
- Take your painkillers just before bed.
- You may find the following sleeping positions helpful:

When can I resume normal activities?
When can I return to work?
You can return to desk-based jobs at approximately 2 weeks following the operation as comfort allows.
Work involving light manual duties, you may be able to return to work at 6 weeks following the operation. However, jobs involving heavy manual labour may take up to 3 months following the operation.
When can I drive?
You can return to driving between 1-2 weeks following the operation, if you are safely able to control the car.
What are the risks and possible complications?
Keyhole surgery is generally very safe. Nevertheless, all operations carry some risks:
Wound ooze: During surgery, sterile salt water is pumped through your shoulder to let the surgeon see clearly inside. Some of this fluid gets absorbed by the tissues and then leaks after the operation. When stained with small amounts of blood it looks pink. This is normal. For this reason, you will have an absorbent pad over your shoulder when you wake up. This will be removed when you go home or the next day.
Anaesthetic risks: Modern surgical practice is very safe, but there are small risks associated with anaesthetics and regional nerve blocks. These risks are increased for those patients with significant pre-existing medical problems. Your anaesthetist will discuss these risks with you.
Deep Infection is very rare after keyhole surgery (<1% risk).
Nerve injury is very rare after this operation (<1risk)
Structural injury in the shoulder is rare and will be dealt with during or after the operation if it occurs.
Post-op blood clots (DVT) are extremely rare after this procedure (less than 1%). You do not normally require any preventative medications for this after sub acromial decompression shoulder surgery.
Wound healing problems: The scar will be over the front of your shoulder. Dissolvable sutures are typically used. It is rare for the wound not to heal nicely, but occasionally this may occur.
Bleeding: This is usually small. It is exceptionally rare to require a blood transfusion. You may see bruising around the shoulder, the front of your chest and down to the elbow. This will subside and should not require any treatment.
Questions
If you have further questions, do feel free to ask your surgeon, who can explain things for you. You will see them the day of your surgery.
Useful Contacts
Heatherwood Hospital:
- Orthopaedic pre assessment 0300 614 7778 / 0300 614 7147
- Arthroplasty Nurse Heatherwood 07789927177
- Nurses Station Treetops Heatherwood 0300 614 4175
- Physio/OT Office Treetops Heatherwood 0300 614 4178
Frimley Park Hospital:
- Frimley Park Physiotherapy 07570 974390
- S2 Elective Ward Frimley 0300 613 3781 / 0300 613 3783
- Elective Helpline Frimley 0300 613 2556
Wexham Park Hospital:
- Ward 1 Wexham Park 0300 615 3010 / 0300615 3012
- Outpatient Physio Wexham 0300 615 3501 / 0300615 3500
- Wexham Park Physiotherapy 07717 199851
Contact us
If you have any queries relating to this information, please contact the Orthopaedics service.
About this information
Service:
Orthopaedics
Reference:
N/027
Approval date:
13 May 2025
Review date:
13 May 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.