Advice after your nerve block for surgery
On this page…
If you need an interpreter, please contact us as soon as possible so that we can arrange for a qualified person to attend your appointments.
What is a PEG?
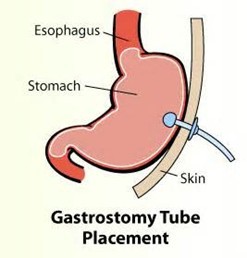
A PEG is a procedure during which a thin tube is placed through the skin of the abdomen into the stomach. The tube can then be used to introduce food, fluids and medicines into the stomach, so you can eat and take medication without swallowing. Since a PEG tube bypasses the throat and gullet, it is given to people who have difficulty with swallowing or for whom there is a risk of food ‘going down the wrong way’ into the lungs.
PEG stands for percutaneous endoscopic gastrostomy.
Percutaneous is the term used for something that is inserted via the skin.
Endoscopic refers to an endoscope, which is the instrument used to carry out the procedure. This is a thin black tube containing a camera and a bright light and is inserted through your mouth and into your stomach.
Gastrostomy refers to an opening into the stomach.
Why do I need a PEG?
The medical team caring for you are concerned that you are not receiving enough nourishment because you are not able to swallow or are having difficulty doing so. It is a safe and effective way of feeding and can easily be removed if it is no longer needed.
If, however, you suffer from reflux or regurgitation of food or acid, it is important to appreciate that these symptoms will not be improved by having a PEG and PEG feeding will not alter the outcome of your underlying disease or condition.
Is there an alternative?
Although sometimes tube feeding can be achieved by passing a thin tube through the nose and into the stomach (nasogastric tube), this method of feeding is more visible, less comfortable and is therefore more suitable for short term use. For people who need to be fed by a tube for more than 4 – 6 weeks, a PEG is more comfortable and easier to manage at home. PEG tubes are also more discreet as they can be tucked away under your clothes. No-one needs to know you have one unless you choose to tell them. If you would like to discuss the options available to you, please speak to a member of your medical team.
Are there any risks involved?
PEG insertion is a skilled procedure and is performed by a highly trained doctor or endoscopy practitioner who takes every care to reduce any risks:
- A perforation (tear) is an extremely rare, but serious, complication that may require surgery.
- Bleeding is a rare complication that does not usually need any further treatment. A small amount of bleeding, noticed in vomit or black stools, is not unusual. This can occur up to several days after the procedure and should not be a cause for concern. If heavier bleeding occurs (equal to more than a cupful), you may require further hospital treatment.
- The use of a sedative drug can, in a very small number of patients (1 in 1,000), cause the breathing or heart rate to slow down. For this reason, the nurse will put a probe on your finger to monitor your pulse and oxygen levels. You might also have your blood pressure monitored. The effects of the sedative are easy to reverse if necessary. If you are asthmatic, or have any breathing difficulties, please inform the nurse on your arrival and bring your inhaler with you if you use one.
- There is also a risk of infection around the site of the tube. Most infections respond well to antibiotics, but the skin and surrounding area need meticulous care at least once a day following the insertion of the tube.
- The insertion of the tube means that there is a tract between the outside skin and the stomach. It takes about 2 - 4 weeks for the tract to seal around the tube. Very rarely the tract fails to heal properly, allowing the contents of the stomach to leak out onto the skin. This will cause irritation and burning due to the high acid level.
There is a small risk that the PEG can become displaced and even accidentally removed. If this happens in initial period after new insertion while the tract is healing, it can cause more serious problems i.e. you can become very unwell with stomach contents leaking inside the abodomen requiring major surgery.
If this happens at home, you should attend your local Accident and Emergency Department as soon as possible for the tube to be replaced. The tract will close very quickly when the tube is no longer there.
It is important that you are aware of and understand the risks before you agree to have a PEG tube inserted. A member of your medical or nursing team will be available to answer any questions that you may have.
What does the procedure involve?
Before the procedure is carried out, you will be asked to sign a consent form once the risks are explained to you. You will not be allowed to eat or drink for several hours before the procedure begins. If you have any other type of tube feeding, it will need to be switched off prior the procedure.
A small needle or cannula will be placed into a vein in your hand or arm. Sedation is given through the cannula. The type of sedation used is called conscious sedation and is not a full general anaesthetic. This means that although you will feel sleepy and relaxed and may not remember the examination, you will still be able to respond to verbal instructions, i.e., you are awake, but drowsy.
A mouth guard will be put into your mouth to protect you from accidentally biting your tongue or the endoscope. The back of your throat may be sprayed with a local anaesthetic to make the procedure more comfortable. An antiseptic solution will be used to clean the skin over your stomach and a local anaesthetic will be used to numb the area where the PEG tube is to be placed.
How is the PEG tube inserted?
The endoscope will be passed through the mouth guard, over the back of the tongue and into the stomach. Saliva and other secretions in your mouth and throat will be removed using suction equipment similar to that used by dentists. The endoscope will allow the endoscopist to see directly into your stomach.
A small incision (cut) is then made through your tummy and the tube will be passed down the endoscope and out through the incision in the abdomen before being secured in place. PEG insertion is mildly uncomfortable and usually takes about 15 minutes.
Preparation
If your appointment is before 1.00pm
Do not have anything to eat or drink from midnight the night before the examination, otherwise food or liquids will obscure the view of the endoscope and the examination will not be possible. You may have a small glass of water no later than 2 hours before your appointment time.
If your appointment is after 1.00pm
Have a very light breakfast before 8.00am. We would recommend toast and a cup of tea. DO NOT eat porridge or eggs. You may have a further drink (without milk) at 10.00am. After that, have nothing to eat until after the examination, although you may have a small glass of water no later than 2 hours before your appointment time.
Special precautions
- If you are an outpatient, please complete the enclosed patient questionnaire and bring it with you. If one is not enclosed, please telephone 0300 615 4157
- If you are asthmatic, please bring your inhalers with you and let the nurse know.
- If you are taking any regular medication for diabetes, please refer to a separate leaflet available by telephoning 0300 615 4157. It explains how to control your blood sugar around the time of your procedure as it is important to maintain a blood sugar above 5 mmol/l. Check your blood sugar level and if necessary suck some glucose tablets ahead of your procedure to achieve this. Please bring your diabetic pills or insulin with you to your appointment.
- For patients on oral anticoagulants (warfarin, apixaban, dabigatran, rivaroxaban) OR the antiplatelet drugs clopidogrel or ticagrelor, we will advise how these medications should be managed around your procedure. Please contact us on 0300 615 4157 if you have not been contacted regarding the above medication.
- If you are taking warfarin, stop taking it 5 days before your procedure. However, if you are taking warfarin for a metallic heart valve, previous venous thrombosis (blood clot) or pulmonary embolism, please do not stop taking it and telephone us on 0300 615 4157 as we will need to make alternative plans to thin your blood around the time of your procedure.
- If you are taking dabigatran, rivaroxaban or apixaban, stop taking it 3 days before your procedure. However, if you are taking the drug for a metallic heart valve, previous venous thrombosis (blood clot) or pulmonary embolism, please do not stop taking it and call us on 0300 615 4157. We will need to make alternative plans to thin your blood around the time of your procedure.
- If you have a heart murmur, have had a heart valve replacement, or suffer from kidney failure, please contact us for advice by telephoning 0300 615 4157.
- Aspirin in low doses is allowed. In the 7 days leading up to the procedure, do not take more than 75mg per day of aspirin.
- If you are taking any other regular medications, please continue these as normal.
- If you have a cough or a cold, please telephone us on 0300 615 4157 as it may be necessary to postpone your appointment.
General information
- It takes 1 - 2 hours for you to be admitted, assessed and for the PEG to be put in place. Afterwards, you will be transferred to another ward.
- Please bring a dressing gown, slippers and something to read.
- Please do not bring any items of value, such as jewellery or credit cards. We cannot accept any responsibility for loss or damage.
What will happen after the procedure?
Once you have recovered from the sedation, you will be transferred to a ward in the hospital to be monitored for 24 to 48 hours.
When the tube is first placed, you may feel a little uncomfortable. This discomfort may be caused by wind and will generally settle after a few hours, though pain killers can be given if needed. Discomfort may also make you reluctant to take deep breaths, but it is important that you do so to help prevent a chest infection. Your throat may also be sore.
Bathing and washing
You can shower 48 hours later, to avoid aiming directly towards the newly inserted tube. You can take a bath only after the wound has healed and tract between skin and stomach is well formed (around 2-3 weeks). The tube end must be closed and you must dry the area thoroughly.
Mouth care
When you are unable to eat it is very important to keep your mouth clean and moist. You should clean your teeth regularly and a mouthwash or artificial saliva spray (Glandosane) can be used if your mouth is dry.
How and when will feeding start?
Your dietitian will have left instructions on the ward for your feeds. These will include the type, amount and rate of infusion. Usually, water is given initially and, if there are no problems, feed will be given the following day.
The feed is given via a pump over several hours or overnight. To prevent heartburn or reflux of feed into your lungs, it is important that you sit up or are well supported by pillows whilst your feed is flowing.
If you have had a PEG inserted because of a swallowing problem, the Speech and Language Therapy Team will review your swallowing from time to time following your discharge.
What about medication?
Where possible the pharmacist will provide all your medications in liquid or dissolvable so as not to block the tube. If this is not possible and you need tablets, you will be given instructions as to how best to manage this.
Medicines are given using a large syringe. You must first flush the tube with at least 30 ml before, in between and after every medication, to adjust the total volume if on quite a few medications.
Who cares for the tube?
Your nurses on the ward will teach you or your carer how to care for the tube before you leave hospital. They will show you how to connect the feeds, clean the skin around the tube and check for any displacement.
Good, frequent care of the tube and site will prevent problems occurring. Tubes can become blocked because of the thickness of the feed and medicines passed through it. The tube requires regular flushing with water and, if done meticulously after every feed and before, after and between every administration of medicine, problems can be prevented.
If the tube becomes worn, split or damaged it will need to be replaced. A tube is changed in the same way as it is inserted and it will usually be possible to use the same tract, avoiding further incisions into the abdominal wall. You and your family members/carers will be trained by specialist nurses called Aboott nurses before you are discharged from hospital.
Who will be available to help with problems?
When you are discharged you will be given contact numbers for help and advice.
Removal
If you no longer require the tube for feeding, it can be removed.
Contact us
If you have any queries relating to this information, please contact the Endoscopy service.
About this information
Service:
Endoscopy
Reference:
H/021
Approval date:
1 June 2026
Review date:
1 June 2029
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.