Advice after your nerve block for surgery
On this page…
This information has been prepared for patients who are undergoing coronary angioplasty/stent insertion at Frimley Park Hospital.
You may have been admitted from the waiting list or are having an angioplasty after being admitted due to angina or a heart attack.
Pre-operative assessment and care
We will invite you to attend a pre-assessment appointment either face to face or as a telephone call, with a Cardiac Nurse Specialist before your procedure.
The nurse will describe the procedure, discuss the risks involved and give guidance on preparing for the procedure, including any changes required to medications, when to stop eating and what to bring with you.
If you take Warfarin or Direct Oral Anti-Coagulants such as Apixaban, Rivaroxaban, Dabigatran or Edoxaban you will be given advice for managing your medication in relation to having the procedure.
If you are diabetic and are taking Metformin tablets you should stop taking the tablets the day before your procedure and restart 3 days after.
Do not stop taking other diabetic medications.
Fasting blood tests
You will be asked to have a fasting blood test, ideally a couple of days before your telephone pre-assessment. We will send a blood form to you with the letter confirming your telephone pre-assessment and procedure appointment.
Appointments for your blood test are booked online via the Frimley Health website.
https://
Aldershot Centre for Health
Farnham Hospital
Frimley Park Hospital – Outpatients
Heatherwood Hospital – Outpatients
King Edward VII Hospital
St Marks Hospital
Wexham Park Hospital – Outpatients
Or alternatively book an appointment with your GP
On the day of your angioplasty +/- stent insertion
- You will be advised at your pre assessment discussion if you need to stop eating before your procedure.
- You should take your usual medication, including blood pressure and water tablets if you take them.
- Please bring in all your medications in original boxes or dosette box with you on the day of the test as you will be taking these as normal.
- Please bring your dressing gown and slippers (or slip on shoes) with you. You will be given a gown to wear for the procedure.
- Please remember to bring your reading glasses with you and something to read or occupy you.
- Avoid bringing any valuables or cash with you, other than small change for a newspaper, as they may be left unattended while you are undergoing your test.
Please be aware that occasionally procedures are delayed or possibly cancelled due to unforeseen emergencies. The ward nurse will keep you informed.
Why undergo coronary angioplasty?
The coronary arteries are around the outside of the heart muscle supplying it with blood and oxygen. In some people these arteries become narrowed and the flow of blood to the heart muscle is reduced.
At times when the heart is working harder, for example during exercise, the reduced blood supply to areas of the heart can cause pain in the chest. This pain is known as angina.
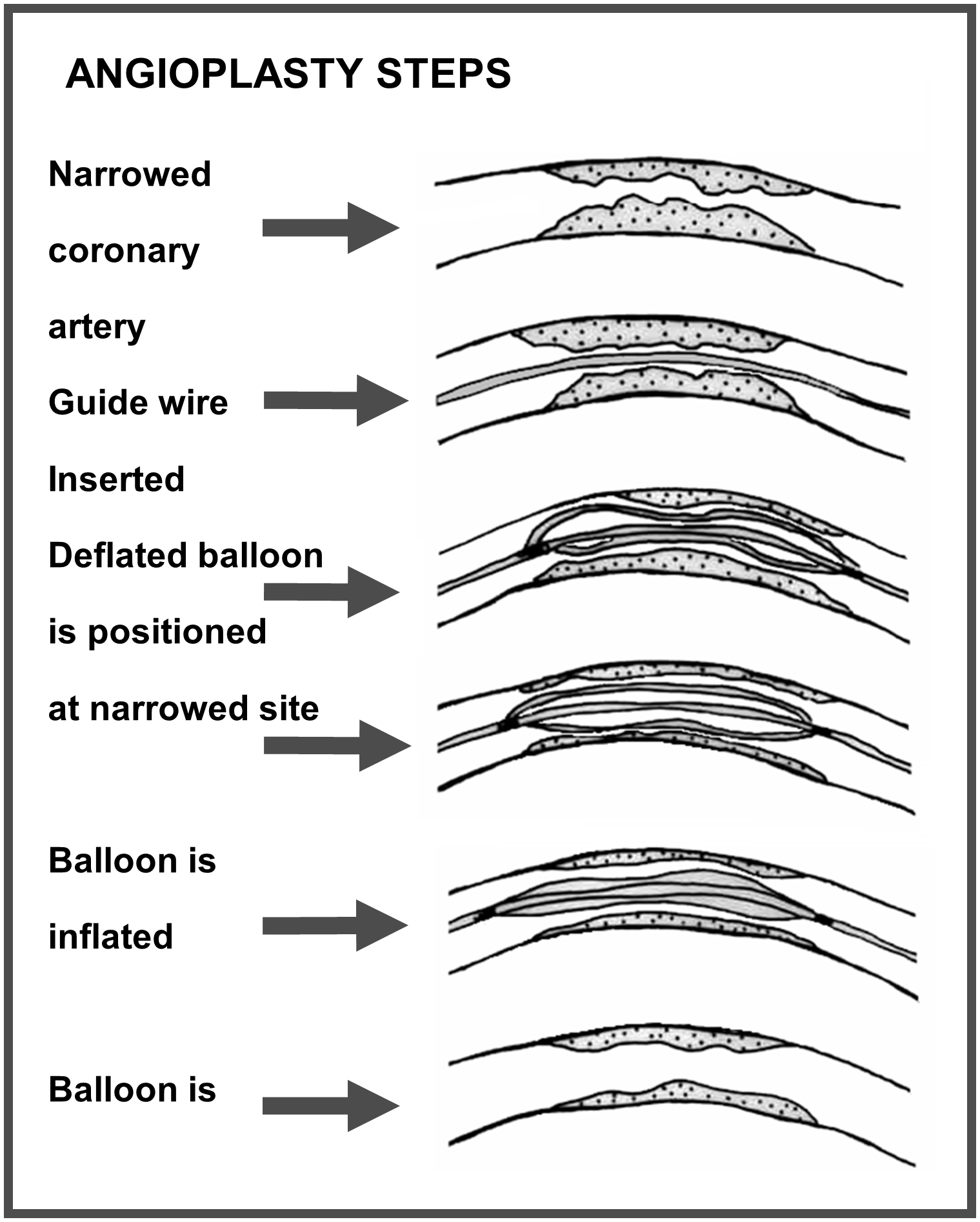
Angioplasty uses a balloon to open a narrowed artery and improve the blood supply to the heart muscle. It is usually done prior to stent insertion but sometimes performed on its own.
Benefits of having coronary angioplasty
The benefits of this procedure are to open the narrowing in the coronary artery and improve blood flow to the heart muscle, thus reducing your symptoms.
Alternatives
Coronary angioplasty is not suitable for all cardiac patients. In situations where the coronary artery disease is not severe medication is an alternative, provided it adequately controls symptoms.
In other situations, an alternative would be cardiac surgery, e.g., Coronary Artery Bypass Graft (CABG).
The angioplasty procedure
The angioplasty procedure is like a cardiac catheter or angiogram. The skin around the chosen site is numbed with a local anaesthetic.
Once the local anaesthetic is effective the doctor inserts a small tube, called a sheath, into the artery. A fine tube, called a catheter, is then passed through the sheath and guided along the artery until it reaches the top of the heart.
As with an angiogram, dye is injected through the catheter and into the coronary arteries to outline them on the X-ray.
Then a very fine guide wire is passed through the inside of the catheter, beyond the catheter end into the narrowed artery.
The doctor will then pass a balloon catheter over the fine guide wire to the site of the narrowing. The balloon is inflated, and this widens the narrowed artery. The balloon is then deflated and withdrawn. Before removing the catheter, the doctor takes some X-ray pictures to see how well the artery has opened.
Stent insertion
A coronary stent is a small stainless steel mesh tube mounted on a balloon catheter. It is introduced into your artery and positioned at the site of the narrowing.
When the balloon is inflated the stent expands and is pressed against the inner walls of the artery. One or more stents may be used in the vessel to span the length of the narrowing. After the balloon is deflated and removed, the stent remains in place keeping the artery open.
The stent is a permanent implant that remains in your artery. It helps hold the artery open, improves blood flow and can relieve symptoms of coronary artery disease, such as angina.
Atherectomy/Shockwave
Sometimes the plaque and calcium is particularly hard or so narrowed that a balloon can’t pass through it. In these cases, Atherectomy or Shockwave may be considered before angioplasty/stent implantation.
Atherectomy
This can take the form of Rotational or Directional Atherectomy.
In Rotational Atherectomy a special catheter, equipped with an acorn shaped diamond tipped drill ‘burr’ is passed over a wire to the site of the blockage. A rotablator system enables the drill to rotate at high speeds to grind away the plaque and calcium. The microscopic particles are washed away in the bloodstream.
With Directional Atherectomy a special catheter with a cutting balloon is used. The catheter is advanced across a guide wire to the blockage site. A low-pressure balloon is inflated which exposes the fine cutter to the plaque. The cutter spins, cutting away pieces of the blockage. These pieces are stored in a section of the catheter and removed after the procedure is complete.
Shockwave
Also known as Intravascular Lithotripsy (IVL), this is a procedure where a lithotripsy balloon is used to crack the hard plaque making it softer and easier to widen. It is similar to lithotripsy used to break up kidney stones. The catheter delivers pulsating energy waves cracking any hardened plaque. The balloon can then be expanded to widen the narrowing.
Procedural Risks
Generally coronary angioplasty is a safe procedure but there can be rare complications.
- In 1 in 100 (1%) of cases patients have an allergic reaction to the contrast dye. This is usually very mild and temporary such as a skin rash.
- In less than 1% of cases it is not possible to stretch the artery and in less than 1 in 500 cases coronary artery rupture can occur. In this event an operation may be needed.
- The risk of heart attack or stroke is less than 1 in 100.
- The overall risk of death is less than 1 in 300 but this can vary with the complexity or urgency of the case.
Care after an angioplasty/stent insertion
After the angioplasty and/or stent implantation you will transfer back to the day ward where the nurses will monitor your heart rhythm and blood pressure very closely and will check the wound site for bleeding. For radial (wrist) procedures you will return to the day ward with a tight band around your wrist. The nurse will reduce the amount of pressure in the band gradually and it will be removed after 3-4 hours.
If your groin is used, you must lie flat until the sheath is removed and you will not be able to bend the affected leg for several hours. Usually, the sheath will be removed around 2 hours after the procedure, but this will depend on your blood test to determine how quickly your blood clots. It is likely that a nurse will need to press on the groin puncture for approximately 10-20 minutes.
If the groin artery has been sealed using an internal closure device, you will be able to sit up directly after the procedure and be on bed rest for 2 hours.
You may eat and drink. It is important to drink plenty of fluids as this will help flush the contrast dye through your kidneys.
Specific advice for those who have had a stent inserted
- You must follow your medication regime exactly.
- Do not stop taking any of your prescribed medications unless you are instructed to do so by the doctor who inserted your stent. Advice should be taken from only this doctor.
- If you experience any side effects of the medications, such as headaches, nausea, vomiting or rash, notify your GP immediately.
- Report any change in angina symptoms, such as severity or frequency, to your GP.
- Attend all appointments for follow-up care, including blood testing.
- Do not have a Magnetic Resonance Imaging (MRI) medical scan within 8 weeks of stent implantation without clearance from your cardiologist.
- Do not use antacids routinely (only use on a one-off basis) unless prescribed by your doctor as they decrease the absorption of aspirin and other medications. If you are using more often, please seek the advice of your GP.
- Do not have any dental work carried out during the first month after your stent insertion as the drugs you are taking may cause bleeding. Please wait until the Clopidogrel course has finished. Should you require emergency dental treatment please inform your dentist.
Visitors
It is the aim of the Cardiac Cath Lab Day Ward (CCL) to ensure that patients have their dignity and confidentiality always respected.
Due to the lack of space and layout in the day ward it is not possible for relatives/carers to stay with the patient throughout the duration of their stay.
However, exceptions can be made should any circumstance arise that the nurse in charge deems appropriate for the carer to stay with the patient.
Relatives/carers may telephone the day ward on 03006 139572
You must arrange for a responsible adult to collect you and drive you home from the Cardiac Catheter Labs after the test. You must not drive for 1 week. You are advised to be off work for a week if a stent has been inserted.
Following the procedure a responsible adult should stay with you overnight.
Going home from hospital
Providing there are no complications you will be going home the same day.
Avoid lifting or strenuous activity for 3 days to ensure artery recovery.
Avoid alcohol for 24 hours to minimise bleeding complications.
If your procedure was done via your groin avoid bending for 3 days. During the first 48 hours, when going up stairs, coughing or sneezing, apply gentle pressure to the groin area to support and prevent wound pain. It is important to avoid constipation, particularly in the first week, as straining can increase pressure on the wound site.
The wound
The site will be covered with a small dressing which you must remove after 24 hours. You may have a shower after 24 hours and it may be easiest to soak the plaster off in the shower. You do not need to replace the plaster. Do not have a bath or use talcum powder for 48 hours. Your wound site may feel tender or be bruised. You may use a painkiller such as Paracetamol but do not take aspirin as a painkiller.
Radial procedures (via the wrist): If the wound bleeds, elevate the arm and apply pressure over the wound site for 5-10 minutes and seek help (GP or 999).
Femoral procedures (via the groin: You may develop a small pea sized lump which should flatten within the next 2-4 weeks. Bruising can extend towards the knee; this may take 2-3 weeks to clear.
Contact your GP if
- the lump feels larger than pea-size
- the bruising gets darker, harder or more painful; or spreads to abdomen and/or buttocks
- or if there is any discharge from the wound site.
If the wound begins to bleed lie down, then you or a responsible adult should press firmly over the wound area for 10 minutes.
Then it is important to contact your GP or call 999.
Medications after your procedure
When you are discharged from hospital, the tablets you are taking may have been changed. If you have any questions about your tablets, please ask before you leave the hospital. You will be given two weeks’ supply of newly supplied tablets to take home but will need to get further prescriptions from your GP.
Aspirin
If you are not taking it already, you will probably be asked to take aspirin. It is important that, unless you are told otherwise, you continue to take your prescribed daily dose.
Clopidogrel
If a stent has been implanted, within 4 weeks the lining of the artery will slowly grow over the stent, incorporating it into the artery wall. Anti-platelet medication (usually called Clopidogrel) will be started prior to the procedure, which you must continue to take until instructed to stop by your consultant.
Your doctor may also prescribe other medications, and it is extremely important that you follow your medication regime exactly.
Chest Pain following your procedure
Following your procedure, you may experience chest discomfort or a bruised sensation. This does not necessarily mean that the angioplasty/stent has not been successful, and it should go away within a few days.
Some patients do get angina pains again after their discharge. If you were using a GTN spray or tablets before your procedure, then you may use these as directed.
|
CHEST PAIN INSTRUCTIONS |
| At the onset of pain, rest for 1-2 minutes. If pain persists, take GTN spray |
|
|
|
If your chest pain is not relieved after 5 minutes take a further dose of GTN spray |
|
|
|
If your chest pain continues for a further 5 minutes take another dose of GTN spray |
|
|
| If you have chest pain despite taking 3 doses of GTN CALL 999 IMMEDIATELY |
To assist your recovery, the quicker you are seen by a doctor, the sooner any treatment required can be started.
Driving post procedure
DVLA guidelines are that you must not drive for at least one week after angioplasty and stent.
If you have had a heart attack and have been successfully treated by angioplasty you may recommence driving after 1 week provided:
- You do not need further urgent angioplasty.
- Your left ventricular ejection fraction is at least 40% prior to hospital discharge.
If not successfully treated by coronary angioplasty, you may recommence driving after 4 weeks from the acute event if there are no other disqualifying conditions.
You do not need to inform the DVLA unless you hold a PSV or HGV licence, but you should inform your insurance company.
If you are a PSV or HGV driver you should inform the DVLA immediately and will be informed not to drive for at least 6 weeks. You will also need to be reassessed by undergoing an Exercise Tolerance Test.
For more information contact the DVLA:
Flying post procedure
Patients who have undergone uncomplicated angioplasty/stent may fly after 1 week, although this should be delayed if the patient has continuing symptoms or is otherwise unstable.
Patients who have suffered an uncomplicated myocardial infarction (heart attack) may fly after 4 weeks. If needed, repatriation may be undertaken after 1 week with the agreement of the airline/doctor.
If there is anything you do not understand or if you would like further information after you have read this information please contact:
- The Cardiac Pre-assessment Team 03006 139575
- Cardiac Cath Lab Day Ward (CCL) 03006 139572
- Cardiac Bookings Office 03006 133344
Useful websites
Additional information can be obtained by logging onto any of the following websites:
Contact us
If you have any queries relating to this information, please contact the Cardiology service.
About this information
Service:
Cardiology
Reference:
C/028
Approval date:
9 January 2025
Review date:
9 January 2028
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.