Advice after your nerve block for surgery
On this page…
The Cornea
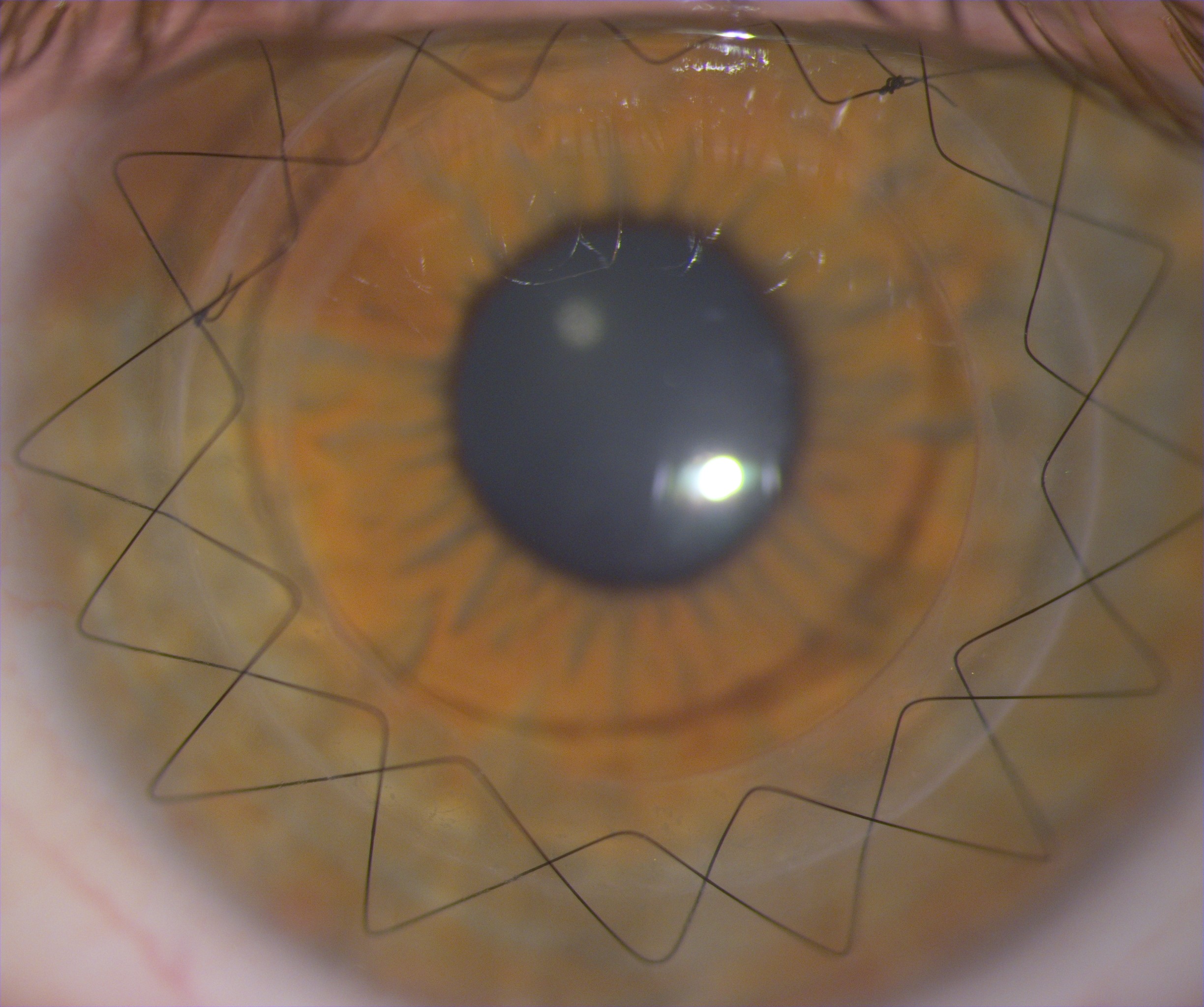
The cornea is the curved window at the front of the eye that must be clear and regular to see. It is part of the focusing system of the eye. It is in front of the iris (the coloured part of the eye) and the pupil (the round black hole in the centre of the iris). The photo below shows a deep lamellar keratoplasty in the first few months after surgery with stitches still in place. A corneal graft is also known as a corneal transplant or a keratoplasty.
What takes place during the operation?
We use a femtosecond laser to make the initial incisions your cornea and the donor cornea. This takes place in a separate laser room and takes about 10 minutes at the start of surgery. We attach a suction clip to your eye, which attaches to the laser. There is a feeling of pressure on the eye during this time. For the rest of the surgery you are usually under general anaesthetic (asleep) for DALK and PK. ALK is a quicker operation and may be done with you awake. A central 8mm diameter disc of cornea is carefully removed from your eye. It is replaced with a matching disc of tissue taken from the donor cornea (this is the corneal graft) and stitched into place with very fine nylon stitches.
How long does the operation take?
Corneal graft surgeries are all day-case surgery, so home later that day.
An anterior lamellar graft (ALK) or full thickness corneal graft (PK) takes about an hour. A deep lamellar graft (DALK) takes about two hours.
Will I need drops after the operation?
Yes. Initially an antibiotic drop and a steroid drop, typically four times a day.
Steroid eye drops are very important to prevent rejection of the graft and continue for a year. After PK we keep you on a low-dose steroid drop forever. It is very important not to run out of steroid drops.
Post-op appointments
You will be seen in the first week after the operation, sometimes on day 1. Your next visit is usually one or two weeks later. We then increase the period between visits, often to two weeks, four weeks, then two months etc. This will depend on the type of operation and each individual.
Things to avoid after the operation
You can do most things but try not to bump the eye. Avoid swimming and strenuous exercise for 3 weeks. It is safe to fly, unless you have been told that air has been used inside the eye during the operation.
Could I catch any disease from the transplant?
The medical history of the donor is checked to exclude the following conditions: rabies, Creutzfeldt-Jakob disease [CJD] and diseases of the nervous system of unknown cause. Blood is taken from all donors to exclude hepatitis B, hepatitis C and HIV. While the cornea is in the Eye Bank it is very carefully examined to reduce the risk of infection with bacteria and fungi; as a result of these checks the risk is tiny. However, because of this tiny risk, once you have had a corneal transplant you will not be able to be a blood or organ donor.
Vision after surgery
This is the big question but unfortunately the answer is difficult. Some lucky patients see very well indeed without glasses with a corneal graft, but unfortunately, they are a minority. Most patients will see well eventually, often well enough to drive, but probably needing glasses, or sometimes even a contact lens. It may take a year or two to get the best vision from the graft. It is all to do with the regularity of the curvature of the graft.
The eye can be left short sighted, longsighted, and a particular problem with grafts is astigmatism. This astigmatism can blur the eye severely and may even need further surgery to correct it. Sometimes it can only be corrected with a contact lens which can be a problem for some patients if the lens is not very comfortable.
When the stitches are removed the vision can change again and so as the glasses prescription.
The corneal stitches
The corneal stitches stay in for several months and even up to 3 years, if left in forever they can cause problems. They are usually removed in the clinic at the microscope. It takes about 10 minutes, with the eye anaesthetised simply with drops.
How long will the graft last?
Most grafts will last for many years. However corneal grafts can fail and become cloudy. The most common cause is corneal graft rejection, and after this corneal endothelial failure (the cells of the cornea fail). Some eyes carry more risk than others. Rejection risk is very low in DALK and ALK.
The 5 and 10 year survival for a PK for keratoconus is 97% and 92% respectively. For all PKs it is 90% and 80%. The figures are better for lamellar grafts.
Trauma Risk
Modern femtosecond laser-cut grafts are structurally stronger than manual grafts. A non-laser cut graft can be ruptured from a blow to the eye. Therefore, contact sports such as football are very risky indeed after a non-laser graft, and even less risky sports like tennis, squash should not be played without good eye protection. A ruptured graft can be disastrous for the eye and lead to blindness. Femtosecond grafts are much safer, but still weaker than an un-grafted eye.
What problems should I seek advice about?
Graft rejection is our main concern (much more common after PK than DALK and ALK). This rejection results from your immune system recognising the graft as being "foreign".
The eye becomes red, sore, sensitive to light, and the vision becomes blurred. This is very treatable, but if not treated early, can lead to permanent graft failure with blurred vision.
Sometimes a stitch becomes loose and it feels like something is in the eye. This also needs to be dealt with quickly as a loose stitch can provoke rejection.
Because each patient is different the above information is a general guide only. A corneal graft can be very successful in restoring lost vision, but should not be undertaken lightly, and involves a great deal of responsibility from both the patient and the surgeon.
Deep anterior lamellar keratoplasty (DALK)
In modern corneal graft surgery, we aim to preserve the layers of your cornea that still work well. In many corneal problems, for example keratoconus, the inner layer of the cornea, the “endothelium” is normal and is best preserved if possible.
In a planned DALK operation we attempt to leave this thin layer of cornea behind and stitch the donor corneal graft on top. We do this because a lamellar graft carries a reduced rejection risk and preserves your healthy endothelium - and both of these mean improved graft survival.
Preserving this thin membrane is a technical challenge, and about 2 in 10 operations will need to be converted to a full thickness graft, because of perforation of the membrane.
Possible complications during surgery
- Severe haemorrhage inside the eye
- This is very rare but can result in the loss of all useful vision from the eye. The risk is less than 1:1000.
- Cataract
- This is also uncommon at the time of surgery but can be caused by injury to the eye's own lens, making it cloudy. Further surgery may then be necessary.
Possible complications following surgery
- Double Anterior Chamber
- Only occurs after DALK, where the graft does not attach to the remaining inner corneal membrane. This can usually be successfully treated with a gas injection into the front of the eye to squash the 2 layers together. This is mostly done in the operating theatre, usually with you awake, and it takes about 10-20 minutes. Sometimes we use stitches too.
- Iris Damage
- Occasionally the pupil may become irregular following surgery or rarely permanently dilated. This happens in the hours after surgery and the eye becomes very painful. It can be reversed if caught early - do not accept very severe pain in the eye following surgery - it should only be a little uncomfortable.
- Endophthalmitis is an infection inside the eye and can be severe. The signs are increasing redness, pain, discharge and reduced vision. Fortunately, it is rare (less than 1:1000 cases) and prompt treatment can help limit any damage. It is most common in the first two weeks after surgery but can occur later, particularly in relation to infection of a loose stitch. Infection can also affect just the graft alone and again is often related to a stitch.
- Glaucoma
- This is when persistently raised pressure in the eye causes some loss of vision. This is more of a problem in patients with pre-existing glaucoma, but not usually a long-term problem for first grafts. More problematic in regrafts. Too much use of steroid drops can cause this problem.
- Corneal Graft Rejection
- This occurs in up to 20% of low risk PKs and up to 80% of high-risk PKs (corneas with abnormal blood vessels or inflammation at the time of surgery). Rejection can be treated well with drops but must be treated promptly. In low risk cases such as keratoconus about 3-5% of grafts will fail in 10 years because of rejection. Rejection is rare in lamellar grafts.
- High Refractive Error
- This can be astigmatism, long-sightedness, short-sightedness, or a combination. The resulting reduced vision is often correctable by spectacles or contact lenses. Occasionally further surgery is necessary to correct this and thereby improve the vision. This takes place after the stitches have been removed.
- Rarely the steroid drops to prevent graft rejection can lead to a cataract.
What problems should I seek advice about?
If your eye becomes red, sore, sensitive to light, and the vision becomes blurred. This is very treatable, but if not treated early, can lead to permanent graft failure with blurred vision. Sometimes a stitch becomes loose and it feels like something is in the eye. This also needs to be dealt with quickly as a loose stitch can provoke rejection.
| From 9am to 5pm Monday to Friday: | 0300 373 5884 |
| From 5pm to 9am and at weekends: | 0300 614 5000 and ask for the eye doctor on call |
Contact us
If you have any queries relating to this information, please contact the Ophthalmology service.
About this information
Service:
Ophthalmology
Reference:
QQ/027
Approval date:
1 May 2025
Review date:
1 May 2028
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.