Advice after your nerve block for surgery
On this page…
What is the aorta?
The aorta is the largest artery (blood vessel) in the body. It carries blood from the heart and descends through the chest and the abdomen. Many arteries come off the aorta to supply blood to all parts of the body. At about the level of the pelvis the aorta divides into two iliac arteries, one going to each leg.
What is an aneurysm and an abdominal aortic aneurysm?
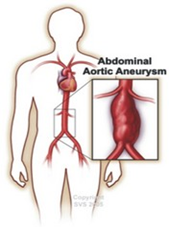
An aneurysm occurs when the wall of a blood vessel is weakened and balloons out. In the aorta this ballooning makes the wall weaker and more likely to burst.
Aneurysms can occur in any artery, but they most commonly occur in the section of the aorta that passes through the abdomen. These are known as abdominal aortic aneurysms (AAA).
What causes an AAA?
The exact reason why an aneurysm forms in the aorta in most cases is not clear. Aneurysms can affect people of any age and both sexes. However, smoking is a major risk factor for AAA with approximately 90% of cases occurring in current or ex-smokers. Conversely, the risk reduces each year following smoking cessation.
There is a strong association between age and prevalence of AAA, with risk particularly increasing after 60 years of age. An AAA rarely ruptures before 65 years of age. Furthermore, an AAA is four to six times more common in men than women.
Your genetic make-up plays a part as you have a much higher chance of developing an AAA if one of your immediate relatives (parent, brother or sister) has or had one. Any female first degree relatives should be checked (scanned) at 60 years of age. Any male first degree relatives should be checked at 50 years of age.
Certain other 'risk factors' increase the chance of getting an aneurysm. These include: smoking, high blood pressure, high cholesterol, emphysema and obesity.
How are aneurysms discovered?
The majority of AAAs cause no symptoms and are discovered by chance in a routine examination by a doctor or by an x-ray or scan for another problem. Less commonly some patients may notice an abnormal pulsation in their abdomen or as the aneurysm stretches it can cause pain in your back or abdomen.
In the UK, there is a one-off screening programme for men aged 65 years and over. This is performed using an ultrasound scan. The aim is to reduce mortality from AAA in men aged 65 to 74 years old. Eligible men are directly invited by the local screening office to one of the clinics. Men aged 65 years and above and who have never undergone screening, can also self-refer. The scan will tell you if there is an aneurysm present and exactly how large it is. If you have been found to have an aneurysm your GP will be informed and you may be referred to your local vascular surgeon or their team.
Here at Frimley you will be offered ultrasound scans to monitor the rate and growth of your aneurysm, depending on its size.
| 2.9cm–3.9cm | 3 yearly |
| 4cm – 4.9cm | Annually |
| 5cm and above | Referred directly to a vascular consultant who will monitor you a little more closely |
| 5.5cm | Referred directly to a vascular consultant who will monitor you a little more closely |
What is the concern about an AAA?
The main concern is that the aneurysm might rupture (burst). The wall of the aneurysm is weaker than a normal artery wall and may not be able to withstand the pressure of blood inside. If it ruptures then internal bleeding occurs which is often fatal. Of course, most AAAs do not rupture - only a certain proportion.
What is the chance of an AAA rupturing?
The chance of rupture is very low for small AAAs. For aneurysms measuring less than 5.5cm in diameter the risk of rupture is less than 1 in 100 per year. As aneurysms get larger than 5.5cm, the risk of rupture increases and it is usually at this size that the option of surgery is considered. For any given size, rupture risk is increased in smokers, those with high blood pressure, and those with a family history of an AAA7.
Each individuals risk from their AAA and from surgery may be
different so any decision on treatment will be carefully considered by your vascular team and always discussed in detail with you and, when appropriate, your family.
What can I do to help myself?
Certain other 'risk factors' increase the chance of a rupture.
Smoking
If you are a smoker the single most important thing you can do to help yourself is to give up smoking7.. Stopping smoking will also help to protect all of your arteries, making it less likely that you will suffer from heart attacks or strokes. Giving up is not easy but there is a smoking cessation service and support groups that can help. Your vascular specialist nurse or GP practice nurse can advise you about these.
Inactivity
Gentle exercise such as walking and cycling are recommended to help to improve your overall level of fitness. Exercise helps your body to produce healthy cholesterol and this helps to protect your arteries against bad cholesterol.
High blood pressure
High blood pressure is a known risk factor for rupture of aneurysms. It is very important that you have your blood pressure checked regularly, at least every 6 months. If you have been prescribed medication for high blood pressure you must make sure that you take it according to the instructions given. Your consultant may want you to take a blood pressure tablet known as a betablocker to reduce you cardiovascular risk.
Diabetes
If you have diabetes it is important that your blood sugar levels are well controlled.
High blood cholesterol levels (fatty substance) in your blood.
You should eat a healthy balanced diet and try to reduce any excess weight. It is important to reduce the level of cholesterol in your blood: you will be given advice on how to do this. Your vascular nurse can refer you to a dietician if needed.
There is evidence that the use of aspirin and a statin reducing major cardiovascular events. Therefore, aspirin and statins is recommended for patients with an AAA to reduce cardiovascular risk.
You may be prescribed a statin drug to lower your cholesterol level and low-dose aspirin to help prevent blood clots from forming.
Statins also reduce the risk of post-operative heart attacks.
Driving with an AAA
If you have a small AAA (<5.5cm) you are allowed to continue to drive. The DVLA should be notified if your aneurysm reaches 6cm in diameter. You are allowed to continue to drive if you have had satisfactory medical treatment and there is no further enlargement of your AAA. If your AAA reaches 6.5cm in diameter you are disqualified from driving.
HGV drivers must tell the DVLA if you have an aortic aneurysm of any size and must not drive if their AAA is > 5.5cm but can resume driving if AAA is successfully treated.
Flying Advice
There is a theoretical increase in the risk of your aneurysm growing if you are a frequent flyer. Whilst we have no objections to you flying when your aneurysm is under 5cm once it reaches 5cm you may find it difficult obtaining travel insurance.
Medications and Surgery
Angiotensin-converting enzyme inhibitors or ACE inhibitors (e.g., Enalapril, Lisinopril or Ramipril) should not be taken on the day of surgery.
Angiotensin II receptor blockers or ARBs (e.g. Candesartan, Losartan or Valsartan) should not be taken on the day of surgery.
Clopidogrel should be stopped 7 days pre-operatively for vascular operations, except for all carotid endarterectomies or unless directed by your consultant.
If you have had a stent inserted into your heart in the last 12 months, please inform your consultant and the decision of when to stop your Clopidogrel will be discussed with a cardiologist.
Warfarin. If you are currently taking Warfarin this will be discussed with you by your consultant, regarding if this needs to be stopped and if you need a covering anticoagulant.
Direct oral anticoagulants or DOAC (e.g. Rivaroxiban, Apixaban or Dabigatran)
This should be stopped at least 48 hours prior to the procedure if high risk of bleeding. If your kidney function is abnormal, this may need to be discontinued for a longer time period prior to surgery. If you take Ticagrelor it will need to be discontinued for 5 days.
Your consultant will advise about this.
Following the procedure, the DOAC will be restarted after 24-72 hours at the discretion of your consultant. You will be started on an anticoagulation injection (e.g. Dalteparin) to help prevent blood clots on the evening of the procedure and daily until the DOAC is restarted. This will be stopped once the DOAC has been restarted.
T.E.D Anti-embolism stockings should never be given for arterial patients unless specifically directed by the consultant, if you are asked to apply a pair please can you question this with a member of the vascular team.
Along with toiletries, night clothes, etc., the vascular team actively
encourages all our patients to bring in day clothes to wear on the
ward whilst an inpatient and to have ready for discharge.
Contact Numbers
If you have any questions or queries you can contact the Vascular Practitioners/Nurse for your area or alternatively the secretary for your Consultant (see page 10).
You may like to look at the following websites for further information. However, as we are not responsible for these websites we cannot endorse them.
| NHS Direct | Tel: 111 Web: www. |
| Abdominal Aortic Aneurysm Quality Improvement Programme |
Tel: 0117 323 2267 Web: www. |
|
Vascular Society of Great Britain and Ireland |
Tel: 020 7973 0306 Web: www. |
| For Help Giving up Smoking: NHS Smoking Help-Line | 0800 169 0169 |
| The Circulation Foundation |
Web: www. Publishes a number of patient information leaflets to help identify and treat vascular illness. It also funds research into the prevention and causes of vascular disease. |
| NHS screening programmes |
Web: www. Includes details of the AAA screening programmes in the various countries of the UK. |
Contact Details
Secretaries at Frimley Park
Mr D J Gerrard, Mr Chong, Mr Chaudary 0300 613 2141
Mr K Jones, Mr Cleanthis, Miss Moore 0300 613 4291
Lt Col Sharrock, Mr Ali, Mr Dastur 0300 613 2487
North Hants Hospital Basingstoke Secretary
Wexham Park Hospital Secretary
Vascular Specialist Nurses
Claire Martin Lead Vascular CNS - FPH 0300 613 6302
Tracey Craig Vascular CNS - FPH
Andrea Croucher Vascular CNS - FPH
Pabita Limbu Vascular CNS - FPH
Kirstie Lane Vascular CNS - WPH 07770702053
Nessa Cababa Vascular CNS - ASPH 07522618600
Contact us
If you have any queries relating to this information, please contact the Vascular surgery service.
About this information
Service:
Vascular surgery
Reference:
Y/036
Approval date:
7 March 2024
Review date:
1 March 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.