Advice after your nerve block for surgery
On this page…
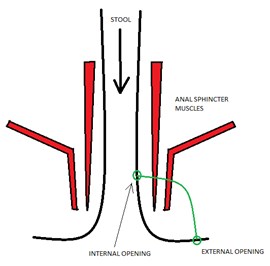
What is an anal fistula?
Two rings of muscle above your anus control your continence. Together, these are the anal sphincter muscles. An anal fistula is an abnormal connection between the inside and outside of the anus/rectum, often passing through one or both anal sphincter muscles. It provides a passage for pus and/or poo to pass to the outside, bypassing the anus. Blockage of this passage can cause an abscess (pain, swelling, feeling unwell).
What are the causes?
They are most commonly caused by infection of the lubricating anal glands. Those that fail to heal, can form a fistula. People with Crohn’s proctitis are especially prone to these problems.
Can it be treated?
Yes, though this can sometimes take time and patience.
Treatment aims are two-fold:
- to treat the symptoms of your fistula
- to maintain your continence.
What are the treatment options?
The first step is to make sure that the fistula can drain. This may need an emergency operation if you are unwell.
Widening of the external opening, cleaning out the tract, and placing a seton can all help this
What is a seton?
A seton is a loose piece of surgical thread that sits in the fistula tract, and helps it to drain. It should be comfortable.
What is a fistulotomy?
This is the mainstay of curative treatment for fistula. A probe is passed down the tract, and a surgical cut is made to divide skin and muscle down to the tract. The tract is cleaned and then allowed to heal. This represents cure in 95% of cases.
Surgeons are careful not to perform fistulotomy if they think there is a chance of impairing your continence. This will depend on the amount and quality of muscle that would be left behind to control your bowel habit.
What is a high fistula?
Where the fistula tract incorporates a lot of muscle, it is termed a “high fistula”. These are not suitable for fistulotomy, as there is a good chance it would impair your long term bowel continence.
There are two safer management options:
- long term seton: Long term setons are safe, and often do not interfere with day-to-day activities. They help to prevent episodes of abscess. They can be turned through 360 degrees to help clear any debris that gets stuck in the tract.
- sphincter sparing procedure: This involves cleaning of the tract, and attempting to close it using heat and sutures. It usually requires a period of time with a seton to prepare the tract. The success rates are usually around 50% each time.
How do I manage at home after the operation?
You will usually be sent home on the same day, with instructions.
- It is likely that you will have local anaesthetic around the wound, so some areas may be numb. This will wear off, and it is important to take regular paracetamol and/or ibuprofen for the first 5 days.
- It is important that you take baths/showers daily. Avoid perfumed soaps or gels, as these can sting. Gently dry the area with paper or a clean towel.
- If your doctor has asked you to “digitate the wound”, when washing, run your finger gently around and in the wound, so that healing occurs from the floor of the cavity up. This avoids formation of a cavity that heals over.
- Wear an absorbent pad in your pants, as the fistula may dribble.
- Avoid adhesive dressings on the skin that block the drainage.
- It is not unusual to get a small amount of fresh bleeding in the days after the operation
- Sometimes the edge of the wound will have tiny stitches. These are keeping the wound open during the days after the surgery, and will fall out or be broken down by the body over time.
Further source of information
NHS website: https://
Contact us
If you have any queries relating to this information, please contact the General surgery service.
About this information
Service:
General surgery
Reference:
Y/049
Approval date:
27 March 2024
Review date:
1 December 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.