Advice after your nerve block for surgery
On this page…
Introduction
Glue ear, or to give it its proper name ‘Otitis Media with Effusion’ is a common condition in children. It can affect any age, but becomes less common after the age of 8 or 9 years.
What is it?
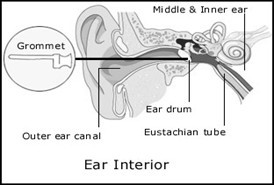
The middle ear is an air containing cavity on the other side of the eardrum.
Air normally gets there via the Eustachian tube which passes from the back of the nose to the middle ear. This tube opens when you yawn or swallow, thus allowing the free passage of air into the middle ear space.
However, in some children, for a variety of reasons, this tube does not work well. This can result in a mild, negative pressure or vacuum in the middle ear and, as a consequence, fluid is drawn into the space from the surrounding tissue – thus you have ‘glue ear’.
The condition is self-limiting in that, as the child grows up, the Eustachian tube begins working properly and the fluid drains away. However, this may not be for many months or even years.
What are the effects of Glue Ear?
- The presence of this thick fluid in the middle ear almost inevitably reduces the efficiency of the hearing mechanism and, therefore, the majority
- Depending on the age of the child, this can have different side effects. Babies and toddlers may be noted to have delayed speech development and, occasionally, disruptive behaviour may result from the child’s frustration. Older children may be noted to have poor hearing by their teachers or it may be noticed at home.
- Alternatively, the hearing deficit may be picked up at one of the various screening hearing checks carried out throughout childhood.
- Apart from hearing difficulties, the other main problem that glue ear can cause is recurrent ear infections. The fluid within the middle ear can act as a good breeding ground for bacteria, and, following a simple cold, an ear infection may develop.
What can be done about Glue Ear?
If the hearing loss or history of ear infection is short-lived, it may be decided to wait a while. During this time family, friends and teachers will have to speak more loudly. Short term treatment with antibiotics or anti allergy therapy may be tried.
A nasal balloon (Otovent) is another option. However, if the problem persists, you may be advised that insertion of grommets is appropriate. Sometimes, the adenoids may be removed as well. A grommet is simply a plastic tube with a hole in it.
Under a brief General Anaesthetic (fast asleep) the grommet is inserted into the eardrum as a day case procedure.
The purpose of this is to allow air into the middle ear. Sometimes the adenoids are removed at the same time.
Following this, your child will be seen from time to time in outpatients until the grommets have fallen out – an average of about twelve months.
Occasionally, once the grommet has come out, the glue ear can recur, requiring a further operation to put grommets in again, but this is unusual.
After leaving hospital:
- Your child may return to normal activities, including school the next day.
- Your child may complain of pain in the ear for a day or two, but it should be mild and easily controlled with Paracetamol.
- No water should be allowed in the ear for the next two weeks, so ear plugs should be worn at bath time.
Can my child go swimming after grommet insertion?
Yes; in most cases but most children should be limited to swimming on the surface of the water as water under pressure will pass through the grommet into the middle ear and may cause infection. You may be advised to use ear plugs.
Risks
- Ear infections: These can occur in children who have grommets. Typically, there is less pain but more discharge. A short course of antibiotics usually clears the Infection, but very rarely the grommet may have to be removed. Generally, antibiotic drops placed into the ear are more effective than antibiotics taken by mouth in this situation.
- Perforation: After the grommet comes out of the eardrum it usually heals up, but very occasionally this doe not happen and a perforation (hole) is left. If it persists further surgery may be required.
If any of these problems arise after you have gone home please contact the wards:
Frimley Park Hospital: Short Stay Surgery ward Direct No: 0300 613 3216
F1 (children’s ward) 0300 613 4252
Please tell the surgeon about all medication you are taking especially warfarin, aspirin and/or the oral contraceptive pill.
Other sources of information:
British Association of Otorhinolaryngologists: www.
National Institute for Health and Clinical Excellence (NICE) www.
Contact us
If you have any queries relating to this information, please contact the Ear or nose and throat (ENT) service.
About this information
Service:
Ear, nose and throat (ENT)
Reference:
G/042
Approval date:
23 February 2026
Review date:
1 February 2029
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.