Advice after your nerve block for surgery
On this page…
Where are your carotid arteries?
The carotid arteries lie in the neck and are the main blood supply to the brain. At a point near the jaw on each side, known as the carotid bifurcation, the common carotid artery divides into the external carotid artery which supplies blood to the face and the internal carotid artery which supplies blood directly to the brain.
The carotid bifurcation is the most common site for carotid artery disease to occur. Arterial disease (atherosclerosis) causes a plaque build-up which then narrows or blocks the carotid arteries. The narrowed carotid arteries may restrict blood to the brain directly, or debris may break off from the carotid plaques and travel in the bloodstream (emboli), passing to the brain or into the artery which supplies the eye.
What symptoms might you experience?
Debris in the arteries passing to the brain may cause a mini stroke or a transient ischaemic attack (TIA). A TIA is often a warning sign, and may be followed by a severe permanent stroke. TIAs usually take the form of a weakness or loss of sensation of the facial muscles, an arm or leg on one side of the body, temporary loss of sight in one eye (amaurosis fugax) or a problem with speaking.
(Remember “FAST” – Facial droop, Arm weakness, Speech defect – Telephone your GP). By definition TIA symptoms last less than 24 hours with the patient making a full recovery. If debris from the carotid plaque travels and blocks the blood supply to that part of the brain, the lack of blood supply can also result in a permanent stroke which may be disabling or fatal.
Why do I need the treatment?
The combination of narrowing of the carotid arteries and a TIA or a stroke puts you at a risk of a major stroke. The greatest risk of a recurrent stroke is shortly after you experience symptoms of a first TIA or stroke and surgery should not be delayed if possible. If you are known to have a significant narrowing of your carotid artery and have had a recent stroke or TIA, you have a significant risk of a further stroke occurring within the next 5 years.
In addition to the medications you may be on to help to protect against further strokes, we know that surgery (Carotid Endarterectomy) will further help to reduce your risk of a future TIA or stroke by 50%.
Diagram of procedure
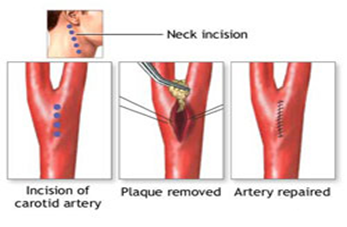
What does carotid endarterectomy surgery involve?
On the morning of the surgery you will have a repeat carotid duplex to confirm that the carotid artery remains patent. If this is not the case the surgery will no longer be necessary and you operation will be cancelled. The sonographer may also mark your neck at this time. The purpose of carotid endarterectomy surgery is to remove the diseased plaque inside the carotid artery and allow greater blood flow to the brain. To do this we have to make a 3-4 inch incision in your neck. The carotid artery is identified and a small cut made in the artery. The plaque is then removed and the artery is then closed, using a patch of synthetic material or sometimes a piece of your own vein. Sometimes the artery can be closed without the need for a patch.
Surgery usually takes around 2 -3 hours to perform and can be done under a local anaesthetic with you awake, or asleep under general anaesthetic. If you choose to have surgery done whilst awake, you will be required to keep very still for the duration of the operation, but the surgeon will be able to talk to you and monitor your brain function. If you choose to have a general anaesthetic, the operation will also require the additional step of using a plastic shunt to ensure that the blood supply to the brain is adequate for the duration of the procedure.
At the end of the operation a drain is inserted this is to reduce the risk of any collection of blood after the operation which may develop into a haematoma.
What are the benefits of surgery?
The key benefit to having a Carotid Endarterectomy performed is reducing your risk of a major stoke in the future. This also assumes that you continue with your other medical treatment with aspirin, cholesterol lowering tablets and blood pressure tablets. Following surgery, you should avoid smoking and maintain a good diet with regular exercise.
Are there any other treatment options besides surgery?
In selected patients who are not suitable for surgery, carotid artery stenting is a less invasive procedure that may be suitable for the treatment of carotid stenosis.
This involves relining the diseased artery from the inside with a new metallic stent. X-Rays are used to guide the introduction of a metallic stent into the groin artery and to position this stent into the carotid artery to maintain blood flow to the brain.
At present, carotid endarterectomy surgery remains the gold-standard surgical procedure with better results compared to carotid artery stenting.
What are the risks of carotid endarterectomy surgery?
The most significant risk to patients is the risk of a further stroke as a result of surgery during the operation or shortly after surgery particularly the first 24 hours. This is in fact uncommon and affects only about 1-3% of patients. There is also a smaller risk of heart attack or death, but this risk is very low at around 1% or less.
There are a number of nerves that run close to the operation site that can be injured. The commonest is a sensory nerve to the upper part of the neck and around the ear. Injury to this nerve can lead to some tingling or numbness in the neck and earlobe, but it is not usually a significant problem. The other nerve commonly seen near the carotid artery is the hypoglossal nerve which controls movement of the tongue. It is occasionally injured or bruised and leads to deviation of the tongue to one side, which often recovers with time.
Occasionally a temporary hoarseness of the voice might develop but it usually recovers with time.
Swallowing difficulties are rarely encountered and may require temporary feeding via a nasogastric tube while function recovers. Rarer nerve injuries involve the nerve supply to the facial muscles of the corner of the mouth causing a weakness resulting in a lop sided smile.
Medications and Surgery
Angiotensin-converting enzyme inhibitors or ACE inhibitors (e.g.,
Enalapril, Lisinopril or Ramipril) should not be taken on the day of
surgery.
Angiotensin II receptor blockers or ARBs (e.g., Candesartan, Losartan or Valsartan) should not be taken on the day of surgery.
Clopidogrel should be stopped 7 days pre-operatively for vascular operations except for all carotid endarterectomies or unless directed by your consultant. If you have had a stent inserted into your heart in the last 12 months, please inform your consultant and this will be discussed with a cardiologist as to the decision of when to stop your Clopidogrel.
Warfarin. If you are currently taking Warfarin this will be discussed with you by your consultant, regarding if this needs to be stopped and if you need a covering anticoagulant.
Direct oral anticoagulants or DOAC (e.g., Rivaroxiban, Apixaban or
Dabigatran) . This should be stopped at least 48hrs prior to the procedure if high risk of bleeding. If your kidney function is abnormal, this may need to be discontinued for a longer time period prior to surgery. If you take Ticagrelor it will need to be discontinued for 5 days.
Your consultant will advise about this.
Following the procedure, the DOAC will be restarted after 24-72 hours at the discretion of your consultant. You will be started on an anticoagulation injection (e.g., Dalteparin) to help prevent blood clots on the evening of the procedure and daily until the DOAC is restarted. This will be stopped once the DOAC has been restarted.
T.E.D Anti-embolism stockings should never be given for arterial patients unless specifically directed by the consultant, if you are asked to apply a pair please can you question this with a member of the vascular team.
Along with toiletries, night clothes, etc., the vascular team actively encourages all our patients to bring in day clothes to wear on the ward whilst an inpatient and to have ready for discharge.
What care will I need after carotid endarterectomy surgery?
After the operation you will be taken to the recovery ward where you will remain under close observation for several hours before being taken back to the ward.
Occasionally, patients are taken to the High Dependency Unit for continued close observation. You will be allowed to eat and drink in the same evening following surgery but care is taken to assess swallowing function before patients resume eating and drinking.
A small drain may be left in your neck at the time of the operation to reduce the risk of any collection of blood. This is normally removed the next day.
When will you be allowed home after surgery?
Patients who do exceptionally well are discharged the next day following carotid endarterectomy surgery. However it is common for most patients to stay in hospital for 24 to 48 hours after surgery.
You should gradually be able to return to normal activities over the next few weeks including light exercise. Your wound may be closed with surgical clips or buried stitches. Your ward nurse will be able to advise you regarding wound care and removal of any skin clips. Skin clips should normally be removed at around 10 days by your GP practice nurse unless advised otherwise by your surgeon.
Research
The Vascular Team at Frimley Health are actively involved in vascular research projects. You may be asked to participate in a research project as a patient if you are felt to be suitable.
Your data may also be used for the National Vascular Registry if you require certain operations or procedures.
Should you have concerns about your personal data and its use, please discuss with your clinician involved in your care. Data is entered automatically to the national database unless you notify us of your dissent.
Any Questions?
If you have any questions about this procedure or treatment, please make a note of them (to ensure you do not forget them) and ask them at your next appointment.
Alternatively you may contact your Consultant via his/her secretary – details are on the opposite page.
Driving
The DVLA advises that patients should not drive for at least 30 days following a TIA (Transient Ischaemic Attack). Following your carotid surgery, we advise you to refrain from driving until you have been seen in our clinic at 6 weeks for a review after your discharge.
Further advice is available from the DVLA (www.
Along with toiletries and night clothes etc. the vascular team would actively encourage all our patients to bring in day clothes to wear on the ward whilst an inpatient to have ready for discharge.
Contact Details
Secretaries at Frimley Park
Mr D J Gerrard & Mr N Dastur: 01276 604772
Mr K Jones & Mr M Cleanthis: 01276 604291
Mr P F S Chong & Mr A Bajwa: 01276 522141
North Hants Hospital Secretary: 01256 313569
Wexham Park Hospital Secretary: 01753 633450
Vascular Specialist Nurses
Claire Martin
Tracey Craig
Andrea Croucher
Katie Fitzcosta
Jean Nixon
01276 526302
or 01276 604604 and ask for bleep 407 / 452 (Frimley Park)
01753 633910 (Wexham Park)
Contact us
If you have any queries relating to this information, please contact the Vascular surgery service.
About this information
Service:
Vascular surgery
Reference:
Y/040
Approval date:
16 August 2018
Review date:
1 April 2021
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.