Advice after your nerve block for surgery
On this page…
What does it involve?
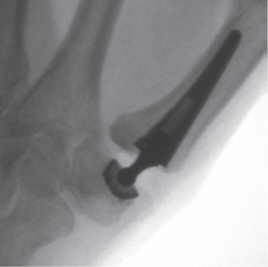
This involves removing the first arthritic joint at the bottom of your thumb and replacing it with an artificial joint.
When is surgery needed?
This operation is performed to relieve pain in the arthritic joint at the bottom of your thumb. Most surgeons would encourage you to try painkillers, splints, activity modification, aids to help with certain tasks (opening jars etc) and steroid injections into the painful joint before considering surgery. The majority of patients with thumb base arthritis can manage their symptoms in this way without ever needing an operation.
Which operation is the right one for me?
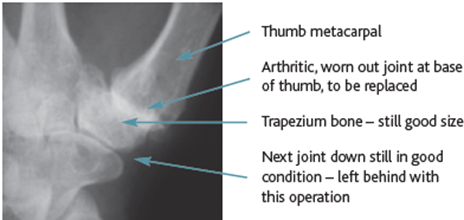
The results from replacing this joint are only just starting to be reliable enough for this operation to be recommended. Your surgeon will discuss other options with you in clinic because of this. To be considered for a replacement of this joint the next joint along should not be arthritic and the trapezium bone must still be big enough for the replacement to sit in (see diagram).
|
Arthritis thumb base joint
|
Thumb CMCJ replacement x-ray
|
|
Thumb joint replacement parts
|
 |
You should read the list of possible complications for this operation carefully and compare them to those for the standard operation for this condition (‘Trapeziumectomy’). It is helpful to consider this type of replacement compared to hip and knee joint replacements. By 10 years after a hip or knee joint replacement most surgeons would be unhappy if less than 98% of their patients did not still have their replacement in place working well. That would mean that 2 in 100 patients would have had to have the joint taken out or re-done for some reason or another. For replacements of the thumb base joint results from modern designs are only just becoming available for up to 5 years after surgery. For these replacements 90% of the joints are now still in and working at that stage. That means that 10 of 100 patients will have had the joint taken out or re-done for some reason by 5 years after their first operation.
These results are reasonable but are not as good as hips and knees yet. Surgeons who offer this sort of joint replacement believe that recovery is slightly quicker with this procedure than a trapeziumectomy and that the function of the thumb is slightly better than with a trapeziumectomy. However, nobody has conclusively demonstrated this yet.
What are the main risks of this operation?
Swelling, Stiffness and Scar pain
This can be reduced by keeping the arm elevated and moving all the free joints as soon as possible. Local swelling around the surgical site can persist for several months. Local swelling can be helped by massaging the tissues and this may also improve any irritability in the surgical scar. Occasionally patients are troubled by more swelling and stiffness than average. In this case complex regional pain syndrome (CRPS) is sometimes the cause. Severe CRPS occurs in less than 1% of cases.
Infection
This is unusual in the hand (less than 1% of cases). Local wound infections can often be treated with oral antibiotics. Rare, deep seated infections may require re-admission to hospital, antibiotics into the vein and occasionally more surgery.
Nerve Damage
The nerves most at risk with these operations are the small branches supplying skin sensation on the back of the thumb and index fingers. The lost patch of skin sensation from these injuries might be irritating but should not affect how your hand works.
Fracture
The trapezium can break apart when it is being prepared for the socket part of the joint replacement. In this case your surgeon would need to convert the operation to a standard trapeziumectomy. Rarely the metacarpal of the thumb could be broken during the operation.
Worsening of Carpal Tunnel Syndrome
Patients with evidence of carpal tunnel syndrome before thumb base surgery may find that these symptoms are much worse around the time of the operation, probably because of increased swelling in the area. Many surgeons would, therefore, consider decompressing the carpal tunnel at the same time as the thumb base surgery if you already have some signs of carpal tunnel syndrome.
Residual thumb base discomfort
No operation for thumb base arthritis is perfect. Some patients will still have some discomfort at the base of the thumb after this operation. This pain may come from scar tissue, from joints next to the replaced joint that are also arthritic or from inflammation around tendons close to the operation site. Usually these symptoms are manageable but occasionally more surgery might be required.
Reduced pinch grip strength (thumb to index finger)
This is likely to be less than in a normal thumb after these operations but more than before the operation, when the joint was very painful. Surgeons who offer a replacement of this joint believe that increased pinch grip strength is one of the advantages of this procedure over simple trapeziumectomy.
Dislocation
The small ball and socket joint used to replace this joint can come apart after this operation (dislocate). This can sometimes be sorted out with a simple manipulation under anaesthesia (pushing ball back into the socket with the hand anaesthetised). Sometimes this doesn’t work and more surgery is needed. Ultimately the replacement can be removed and a trapeziumectomy carried out if necessary.
Loosening of components
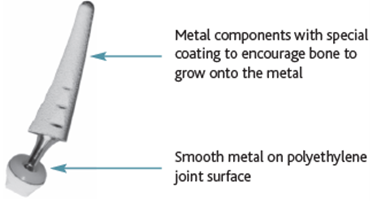
In the past this has been a big problem with these replacements. The socket part of the joint is small and sits in a small bone, the trapezium. This part has loosened most often in the past. Modern designs use a special surface on the metal implant to encourage your bone to ‘grow’ onto the surface of the implant. That makes loosening less likely. It takes a bit of time for the bony growth to get strong which is why we recommend that very heavy loading of the new joint is limited for the first 3 months after your operation. If the components do become very loose more surgery might be required.
Post Operative Course
Day 1-14
- A dressing and padded bandage with a plaster is applied after the operation;
- Keep the dressings clean and dry;
- Keep the arm elevated in a sling or on pillows to reduce swelling;
- Start moving all the joints that are not immobilised as soon as possible to prevent stiffness;
- Take painkillers before the anaesthetic wears off and as necessary thereafter.
2-3 weeks
- An appointment will be made for you to see the hand therapy team;
- They will check your wound and make you a removable splint and start further rehabilitation.
3 months
- By this stage most people will have returned to most activities.
- Hand therapy will continue if needed.
Plaster Cast Information
Contact your surgical centre if:
- Your fingers become blue, swollen or numb and tingling with a plaster cast in place;
- You see any discharge, wetness or detect any unpleasant smells from around your cast;
- The cast becomes cracked, soft, loose or uncomfortable.
Outside normal working hours you may need to attend your local Accident and Emergency Department for help with these issues.
Driving
You may drive when you feel confident to control the car, even in an emergency. For this surgery, it can be up to two months before many people feel this confident. The Hand Therapy team will discuss this with you in more detail. You should discuss it with your insurer if you are considering driving with a splint in place.
Time off Work
This will vary depending on the nature of your job. ‘Fit for work’ notes can be provided on the day of your operation, at your clinic visits and by your own GP.
Contact us
If you have any queries relating to this information, please contact the Orthopaedics service.
About this information
Service:
Orthopaedics
Reference:
N/064
Approval date:
19 August 2024
Review date:
1 July 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.