Advice after your nerve block for surgery
On this page…
Introduction
The aim of this leaflet is to give you a general understanding of shoulder instability and what happens before and after your shoulder stabilisation surgery. It is designed to help you to prepare for your operation and after care once you go home.
The shoulder
The shoulder is the most mobile joint in the human body. It is formed between the ball shaped bone and the top of your arm (humeral head) and a nearly flat surface on the shoulder blade that forms a socket (the glenoid).
The joint relies heavily on the surrounding muscles (the rotator cuff), a rim of cartilage on the glenoid (the labrum) and surrounding ligaments and capsule to maintain its stability.
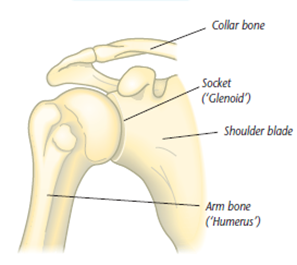
Figure 1: Diagram of the bones of the shoulder.
Shoulder instability – what is it?
Shoulder instability can occur after a shoulder dislocation, particularly in people under the age of 25. Dislocations are more common in younger patients and are often a result of injury, such as when playing contact sports. Symptoms of instability can include pain, reduced movement due the shoulder feeling unstable and repeated dislocations or ‘subluxations. Most dislocations are forwards and/or downwards. Approximately 10% of dislocations are backwards. Dislocations can result in damage to the cartilage (labrum) causing it to separate from the bone. The ligaments and capsule surrounding the joint can also become stretched or torn, resulting in the shoulder becoming unstable.
The aim of the surgery is to repair the structural damage in your shoulder. This coupled with physiotherapy rehabilitation after your operation will help you return to your work and usual activities without the feeling of instability.
Younger patients (under the age of 25) are more likely to require surgical stabilisation of the shoulder, whereas older patients may be able to manage their instability with physiotherapy.
Information about the procedure
Arthroscopic stabilisation
You have been listed for arthroscopic (keyhole) stabilisation surgery which will aim to repair the labrum and re-tension the shoulder joint.
The surgery is under a general anaesthetic and usually a regional nerve block to your arm. The labrum is repaired via sutures and anchors which allows the loose joint to be re-tensioned. The anchor material is usually ‘bio composite’ meaning it will slowly be replaced with bone over time.
You will have 2-3 tiny scars on the front and the back of the shoulder.
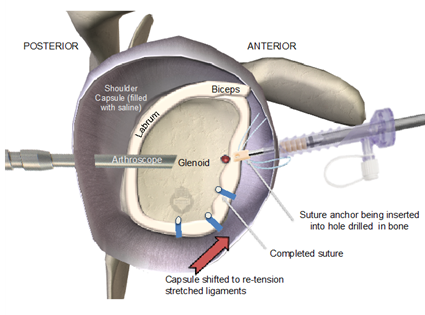
Figure 2: Diagram to show surgical repair of labrum and capsule of the shoulder.
What happens before your admission to hospital?
You will be contacted by the bookings team to arrange your surgery date. You will need to attend the pre-operative assessment clinic to assess your fitness for surgery.
At the time of listing for surgery, you will have been given information regarding your surgery, and an opportunity to ask questions. This information leaflet should also help you to understand the pathway.
We recommend you source Benzoyl Peroxide 5% gel from your pharmacist. This is an over-the-counter acne cream. You should rub a pea sized amount over the front of your shoulder and towards your armpit once a day for the three days prior to your operation. This has been shown to reduce levels of a certain bacteria that sometimes causes infection in shoulder surgery.
Coming into hospital
You will be told when to arrive at the hospital on the day of your surgery. Please do come on time so we can get you ready in time for your operation.
Please do not eat any food for 6 hours prior to your surgery. You can drink water until your surgery. You may be given a small carbohydrate drink 2 hours prior to your surgery when you are with us.
You will normally go home on the same day as your surgery. There are many advantages to being in your own environment, reducing the risk of complications and being in control of your own recovery. In some rare cases, your consultant may ask you to stay overnight and go home the following morning. If this if required, you will be made aware of this prior to your admission.
You will need to arrange for someone (e.g. a family member or a friend) to bring you to and from the hospital as you will not be able to drive home after your operation.
What do I need to do after my surgery?
Pain relief
A regional nerve block is sometimes used during surgery which means your limb may feel numb immediately after your operation. It is normal to feel some pain as the block wears off and you will be provided with some painkillers to help with this. It is important to take your painkillers as prescribed to keep pain to a minimum. If you are struggling with pain post operatively and it is impeding your ability to sleep or be comfortable, please get in touch with the nursing team on 0300 614 4130 / 0300 314 4131.
Ice
Ice can be helpful to reduce pain/swelling. Protect your dressings from getting wet with a plastic bag. Wrap a bag of ice/frozen peas in a damp towel and apply for 10-15 minutes. This can be repeated every 3-4 hours.
Wound care
Following your operation, you will usually have a few very small wounds these will be covered with a dressing.
Your wounds will need to be kept clean and dry until they have healed (usually about 10 days). The nursing staff will provide you with more information about wound care on discharge. At 2 weeks after your operation, you will attend a nurse physio/led clinic for your wound to be checked.
Rehabilitation
A physiotherapist will see you on the day of your operation to go through some early exercises and sling use with you. You will also be seen by a physiotherapist to monitor progress at your week 2 review.
You will be given an appointment for outpatient physiotherapy to start at 4-6 weeks post operation. At this stage you will be able to remove your sling. It is vital that you work with your therapist to maximise the outcome of your surgery. Your therapist will check how you are progressing with your exercises but will also help you to regain your motion. You will be given a separate handout with your exercises on.
Sleeping positions
Sleep is important in your recovery and can be a bit of a challenge after an operation. Here are some tips that may help.
- Take your painkillers just before bed.
- You may find the following sleeping position helpful - use a pillow behind your arm when asleep.

When can I resume normal activities?
When can I return to work?
If you have a desk job, you can return to work when you feel ready using the sling. If you have job that requires heavy lifting/duties, you will be signed off for at least 3 months.
When can I drive?
You can normally return to driving at 6-8 weeks.
When can I return to sporting activities?
Your physiotherapist will give you guidance on this throughout your rehabilitation as your mobility and strength improves. You will be off contact sports for at least 6 months.
What are the risks and possible complications?
Arthroscopic stabilisation specific complications
Re-dislocation or on-going instability symptoms - studies report failure rates between 5 and 15% for this surgery at two years – this may include a repeat injury (e.g another rugby tackle). If you continue with contact sports, you may re-injure a successfully stabilised shoulder. The risk is higher in teenagers and those with a history of multiple pre-operative dislocations.
Stiffness (5%) – this rarely requires surgery as the tightened soft-tissues 'stretch out' over time.
On-going pain. Occasionally patients notice on-going twinges of pain in their shoulder, despite it being stable and functioning well.
Uncommon (1-2%)
Infection
Infection around a joint is a serious complication. It is therefore important that you do not have any infections prior to surgery, for example, skin, chest or urinary tract infection. Should you have an infection prior to your surgery, please inform the pre-assessment staff.
Wound healing problems
If you have a shoulder stabilisation you will have a small incision at the front and the back front of your shoulder. Dissolvable sutures are typically used. It is rare for the wound not to heal nicely, but occasionally this may occur. If you notice excess discharge, an offensive odour, or surrounding redness then please contact the nursing team on 0300 614 4130 / 0300 614 4131.
Anaesthetic risks
Modern surgical practice is very safe, but shoulder stabilisations require a general anaesthetic and normally a nerve block (to numb the whole arm to reduce peri-operative pain). There are small risks associated with anaesthetics and these risks are increased for those patients with significant pre-existing medical problems. The nerve block is also very safe and the risks of these will be explained to you by the anaesthetist.
Rare (less than 1%)
Major bleeding
Normally there is minimal blood loss during this operation. It is extremely rare to require a blood transfusion. You may see bruising around the shoulder, the front of your chest and down to the elbow. This will subside and should not require any treatment.
Nerve injury
Whilst rare, injury to the nerves around the shoulder can occur during surgery. If nerve injury does occur, it may cause weakness of the shoulder or arm muscles. Normally, nerve injury is the result of a stretch to the nerves and will recover with time; but permanent injury can (very rarely) occur.
Fracture
This is very rare. If an event did occur, your surgeon would normally be able to deal with it during the operation.
Post-op blood clots (DVT)
The risk is very low (less than 1%) and is reduced as much as possible by early mobilisation, compression device pumps and exercises. We do not normally prescribe blood thinners for patients undergoing a stabilisation procedure.
Questions: If you have further questions, do feel free to ask your surgeon, who can explain things for you. You will see them on the day of your surgery.
Useful Contacts
Heatherwood Hospital:
- Orthopaedic pre assessment 0300 614 7778 / 0300 614 7147
- Arthroplasty Nurse Heatherwood 07789927177
- Nurses Station Treetops Heatherwood 0300 614 4175
- Physio/OT Office Treetops Heatherwood 0300 614 4178
Frimley Park Hospital:
- Frimley Park Physiotherapy 07570 974390
- S2 Elective Ward Frimley 0300 613 3781 / 0300 613 3783
- Elective Helpline Frimley 0300 613 2556
Wexham Park Hospital:
- Ward 1 Wexham Park 0300 615 3010 / 0300615 3012
- Outpatient Physio Wexham 0300 615 3501 / 0300615 3500
- Wexham Park Physiotherapy 07717 199851
Contact us
If you have any queries relating to this information, please contact the Orthopaedics service.
About this information
Service:
Orthopaedics
Reference:
N/068
Approval date:
13 May 2025
Review date:
13 May 2027
Click ‘show accessibility tools’ at the bottom of the page

Then click ‘select language’
![]()
Alternative formats
You can use the accessibility toolbar at the bottom of your screen to:
-
Change the text size
-
Adjust the font
-
Modify the colour contrast
-
Use the translate function
If you would like this information in another format, such as Braille, audio, or easy read, please speak to a member of staff.
You can also print as well as download as PDF using the “Print this page” button at the end of the page.
Staff will print a copy for you on request
Important note
This page provides general information only. It is developed by clinical staff and is reviewed regularly every 3 years for accuracy. For personal advice about your health, or if you have any concerns, please speak to your doctor.